by Jason Wasserman MD PhD FRCPC
May 23, 2023
What is squamous cell carcinoma in situ of the oral cavity?
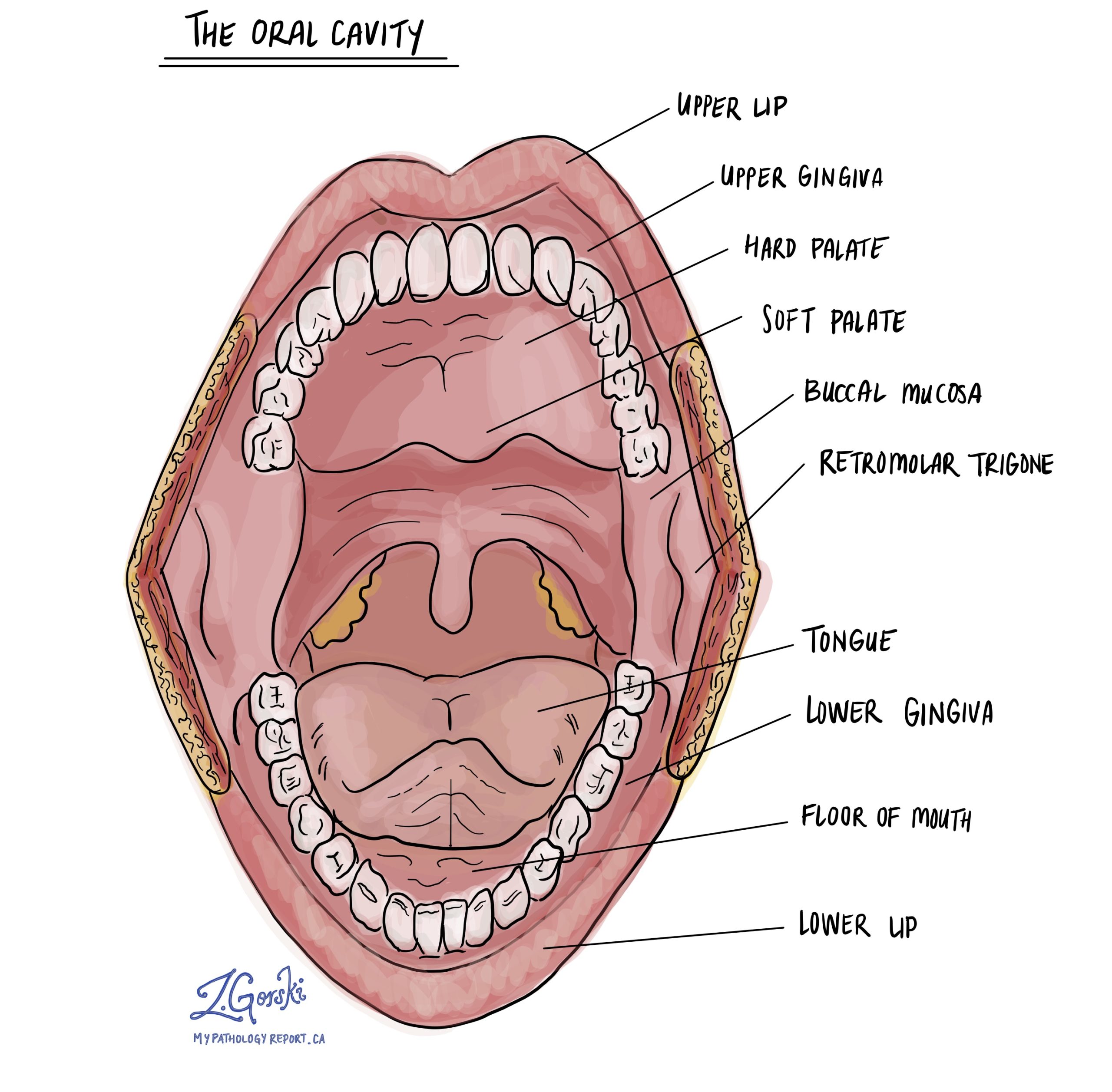
Squamous cell carcinoma in situ (CIS) is a non-invasive type of oral cavity cancer. The oral cavity includes the lips, tongue, floor of mouth, cheeks, and hard palate. If left untreated, squamous cell carcinoma in situ is associated with a high risk of developing a type of invasive oral cavity cancer called squamous cell carcinoma. Another name for squamous cell carcinoma in situ is severe keratinizing squamous dysplasia.
What causes squamous cell carcinoma in situ in the oral cavity?
The most common cause of squamous cell carcinoma in situ in the oral cavity is smoking. Other causes include excessive alcohol consumption, immune suppression, and inflammatory conditions such as lichen planus.
What are the symptoms of squamous cell carcinoma in situ of the oral cavity?
Symptoms of squamous cell carcinoma in situ in the oral cavity include pain and bleeding. The area of the oral cavity involved may appear red or white.
Why is squamous cell carcinoma in situ called “non-invasive”?
Squamous cell carcinoma in situ of the oral cavity is called non-invasive because the tumour cells are located entirely within a thin layer of tissue on the inside surface of the oral cavity called the epithelium. This is the same location where healthy squamous cells are normally located. In contrast, a tumour is considered “invasive” if the tumour cells spread into the stroma below the epithelium.
Is squamous cell carcinoma in situ of the oral cavity considered malignant?
Squamous cell carcinoma in situ of the oral cavity is not considered malignant because the tumour cells are not able to spread to other parts of the body.
Can the tumour cells in squamous cell carcinoma in situ spread to other parts of the body?
No. Because squamous cell carcinoma in situ is non-invasive, the tumour cells are unable to spread to other parts of the body.
How is the diagnosis of squamous cell carcinoma in situ in the oral cavity made?
The diagnosis of squamous cell carcinoma in situ in the oral cavity is usually made after a small sample of tissue is removed in a procedure called a biopsy. The biopsy is usually performed because you or your doctor saw an abnormal-looking area of tissue within your oral cavity. Your pathology report will probably say what part of the oral cavity was sampled in the biopsy. The diagnosis can also be made after a larger piece of tissue is removed in a procedure called an excision.
What does squamous cell carcinoma in situ of the oral cavity look like under the microscope?
Squamous cell carcinoma in situ starts from specialized squamous cells in a thin layer of tissue called the epithelium. When examined under the microscope, the abnormal cells in an area of squamous CIS are usually larger than normal, healthy squamous cells. The cells may be described as hyperchromatic as the nucleus (the part of the cell that holds the genetic material) is often darker than normal. Large clumps of genetic material called nucleoli may also be seen in the nucleus of the abnormal cells. These squamous cells also undergo an abnormal pattern of development which results in a process called keratinization.

What is a margin and why are margins important?
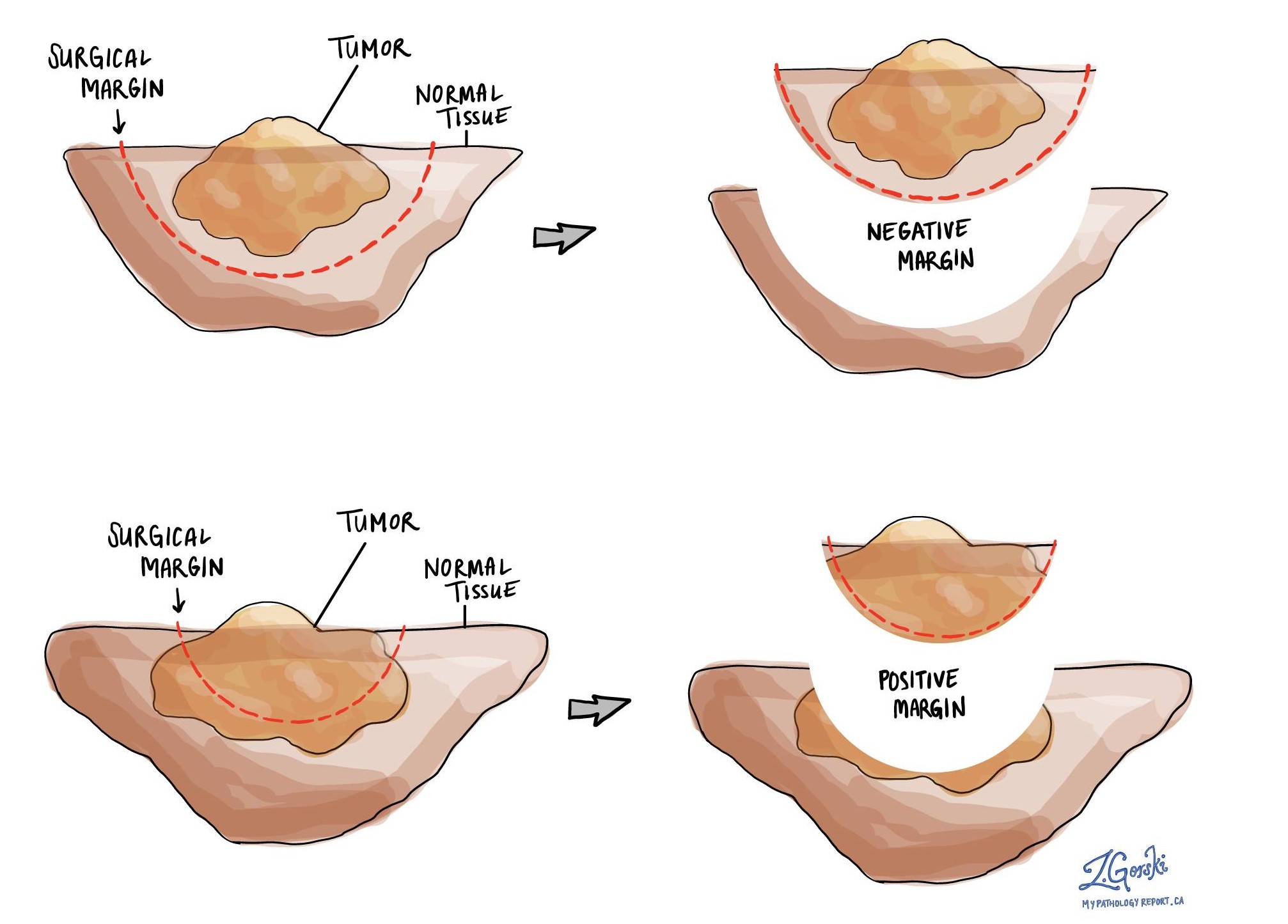
A margin is any tissue that was cut by the surgeon in order to remove the area of squamous cell carcinoma in situ from your body. The types of margins described in your report will depend on the area of the oral cavity involved and the type of surgery performed. Margins will only be described in your report after the entire abnormal area of tissue has been removed.
A negative margin means that squamous cell carcinoma in situ was not seen at any of the cut edges of tissue. A margin is called positive when there is squamous cell carcinoma in situ at the very edge of the cut tissue. A positive margin is associated with a higher risk that squamous cell carcinoma in situ or squamous cell carcinoma will come back at the same site after treatment.

Do you have a question about your pathology report?
Our team of experts is here to help.
Ask a Pathologist.
Our work is generously supported by:
![]()