

by Jason Wasserman MD PhD FRCPC
November 24, 2023
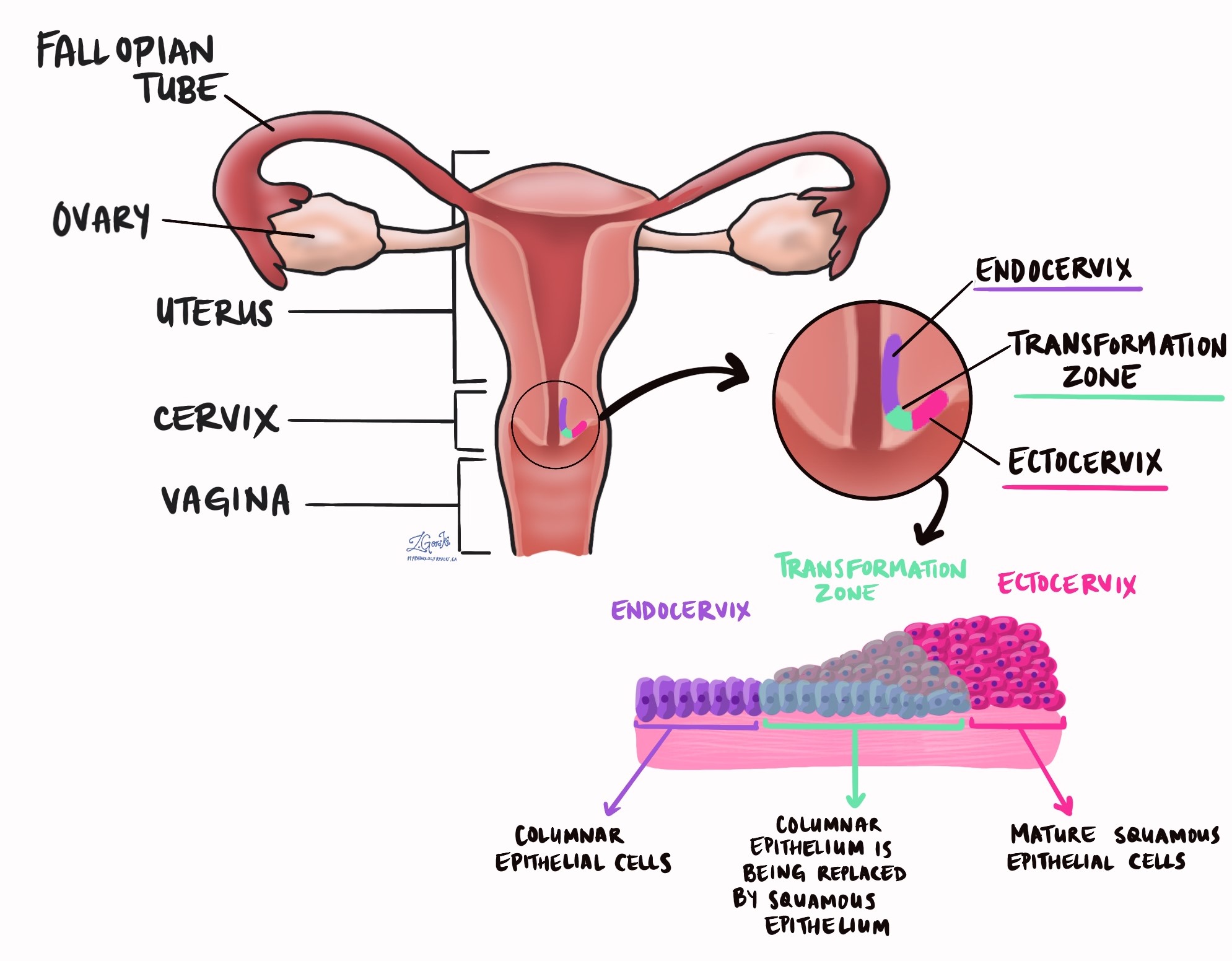
Adenocarcinoma is a type of cervical cancer. It develops from columnar cells normally found on the surface of the endocervix. Most tumours start from a non-invasive type of cancer called endocervical adenocarcinoma in situ (AIS).
What are the symptoms of adenocarcinoma of the cervix?
The most common symptom of adenocarcinoma of the cervix is abnormal uterine bleeding. Less common symptoms include pelvic pain and pressure.
What causes adenocarcinoma of the cervix?
The most common cause of adenocarcinoma of the cervix is infection with high-risk types of human papillomavirus (HPV), specifically types 16, 18, and 45. These tumours account for about 80 to 85% of cases worldwide. At present, doctors do not know what causes the other 15 to 20% of cases that are not associated with HPV.
Your pathology report for adenocarcinoma of the cervix
The information found in your pathology report for adenocarcinoma of the cervix will depend on the procedure performed. For small procedures such as a Pap smear, your report may only include the diagnosis. A biopsy report may also include the tumour grade and immunohistochemistry may be performed to look for p16 in the tumour cells. For larger procedures such as an excision or resection performed to remove the entire tumour, additional information such as the size of the tumour, depth of invasion, and the assessment of margins may also be described. Please see the sections below for more details.
What is p16 and why is it important?
Cells infected with high-risk types of HPV typically produce large amounts of a protein called p16. Pathologists can see this protein inside cells by performing a test called immunohistochemistry. When immunohistochemistry is performed, most adenocarcinomas of the cervix are positive for p16. As a result, this test is used to confirm the diagnosis of adenocarcinoma and rule out other conditions that can look like adenocarcinoma under the microscope.
What does it mean if adenocarcinoma of the cervix is described as well differentiated, moderately differentiated, or poorly differentiated?
Pathologists divide adenocarcinoma of the cervix into three grades based on how much of the tumour is making glands similar to those normally found in the cervix. The three grades are called well differentiated, moderately differentiated, and poorly differentiated. The differentiation of the tumour is important because less differentiated tumours (for example, those that are poorly differentiated) tend to grow faster and are more likely to metastasize (spread) to other parts of the body such as lymph nodes.
How do pathologists determine the tumour size for adenocarcinoma of the cervix and why is it important?
After the tumour has been surgically removed, it will be measured in three dimensions – length, width, and depth of invasion. Tumours with a depth of invasion greater than 5 mm and a width greater than 7 mm are more like to metastasize (spread) to other parts of the body such as lymph nodes. These measurements are also used to determine the pathologic tumour stage (pT).
- Length – The tumour is measured from top to bottom.
- Width – The tumour is measured from side to side.
- Depth of invasion – The tumour is measured from the epithelium on the surface of the cervix to the cancer cells at the very deepest point of invasion.
What does tumour extension mean and why is it important?
Adenocarcinoma starts within the cervix however larger tumours can grow to involve nearby organs such as the endometrium, vagina, bladder, or rectum or supporting tissues such as the parametrium. Pathologists use the term tumour extension to describe how far the cancer cells have spread from their starting point in the cervix into surrounding organs and tissues. Tumour extension into other organs or the parametrium around the cervix is important because it is associated with a worse prognosis and is used to determine the pathologic tumour stage (pT).
What does stromal invasion mean and why is it important?
The tissue that covers the inside surface of the cervix is called the epithelium while the tissue just below the epithelium is called the stroma. Adenocarcinoma of the cervix starts in the epithelium but as the tumour grows, the cells spread into the stroma. This is called stromal invasion. The amount of stromal invasion is not the same as the tumour size because the tumour size also includes any AIS that may be above the area of invasion. For that reason, the size of the tumour may be larger than the amount of the stromal invasion.
Most pathology reports will describe the amount of stromal invasion in two directions:
- Depth of invasion – This is the amount of invasion measured from the surface of the tumour to the deepest point of invasion.
- Horizontal extent of invasion – This is the amount of invasion measured from one side of the tumour to the other.
The amount of stromal invasion is important because it is used to determine the pathologic tumour stage (pT). In general, less stromal invasion is associated with a better prognosis while more invasion is associated with a worse prognosis.
What does lymphovascular invasion mean and why is it important?
Lymphovascular invasion means that cancer cells were seen inside a blood vessel or lymphatic vessel. Blood vessels are long thin tubes that carry blood around the body. Lymphatic vessels are similar to small blood vessels except that they carry a fluid called lymph instead of blood. The lymphatic vessels connect with small immune organs called lymph nodes that are found throughout the body. Lymphovascular invasion is important because cancer cells can use blood vessels or lymphatic vessels to spread to other parts of the body such as lymph nodes or the lungs.

What are lymph nodes and why are they important?
Lymph nodes are small immune organs found throughout the body. Cancer cells can spread from a tumour to lymph nodes through small vessels called lymphatics. For this reason, lymph nodes are commonly removed and examined under a microscope to look for cancer cells. The movement of cancer cells from the tumour to another part of the body such as a lymph node is called a metastasis.

Lymph nodes examined are usually divided into those found in the pelvis and those found around a large blood vessel in the abdomen called the aorta. The lymph nodes found around the aorta are called para-aortic. Lymph nodes on the same side as the tumour are called ipsilateral while those on the opposite side of the tumour are called contralateral.
If any lymph nodes were removed from your body, they will be examined under the microscope by a pathologist and the results of this examination will be described in your report. Most reports will include the total number of lymph nodes examined, where in the body the lymph nodes were found, and the number (if any) that contain cancer cells.
If cancer cells are found in a lymph node, the size of the area involved by cancer will be measured and described in your report.
- Isolated tumour cells – The area inside the lymph node with cancer cells is less than 0.2 millimetres in size.
- Micrometastases – The area inside the lymph node with cancer cells is more than 0.2 millimetres but less than 2 millimetres in size.
- Macrometastases – The area inside the lymph node with cancer cells is more than 2 millimetres in size.
The examination of lymph nodes is important for two reasons. First, this information determines the pathologic nodal stage (pN). Second, finding cancer cells in a lymph node increases the risk that cancer cells will be found in other parts of the body in the future. As a result, your doctor will use this information when deciding if additional treatment such as chemotherapy, radiation therapy, or immunotherapy is required.
What does it mean if a lymph node is described as positive?
Pathologists often use the term “positive” to describe a lymph node that contains cancer cells. For example, a lymph node that contains cancer cells may be called “positive for malignancy” or “positive for metastatic carcinoma”.
What does it mean if a lymph node is described as negative?
Pathologists often use the term “negative” to describe a lymph node that does not contain any cancer cells. For example, a lymph node that does not contain cancer cells may be called “negative for malignancy” or “negative for metastatic carcinoma”.
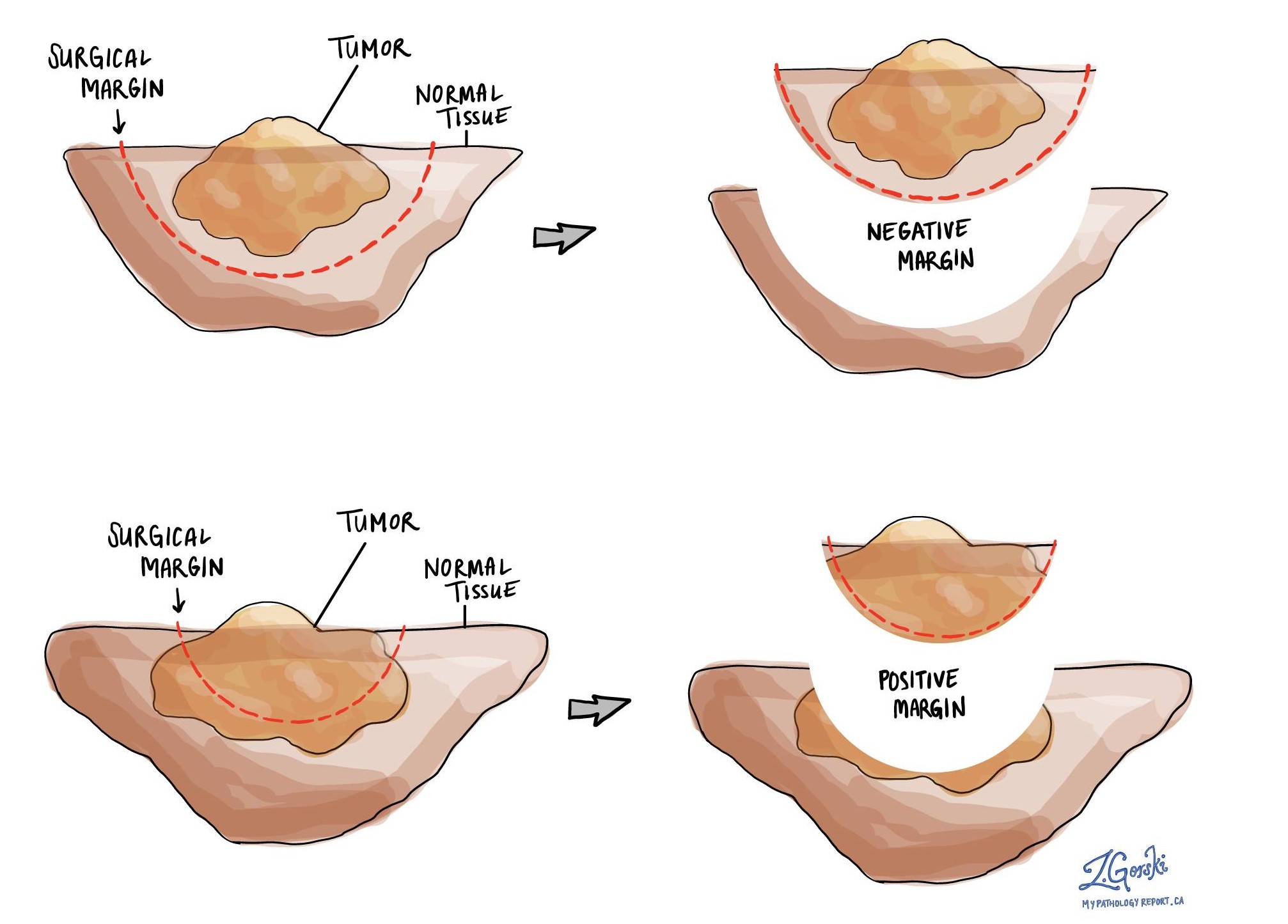
What is a margin and why are margins important?
A margin is any tissue that has to be cut by the surgeon in order to remove the tumour from your body. If you underwent a surgical procedure to remove the entire tumour from your body, your pathologist will examine the margin closely to make sure there are no cancer cells at the cut edge of the tissue. A margin is considered positive when the cancer cells are seen at the edge of the cut tissue. If AIS is seen at the margin that will also be described in your report. Finding cancer cells at the margin increases the risk that the tumour will grow back in that location.
The number and type of margins described in your report will depend on the type of procedure performed to remove the tumour from your body. Pap smears do not have margins.
Typical margins include:
- Endocervical margin – This is where the cervix meets the inside of the uterus.
- Ectocervical margin – This is the bottom of the cervix, closest to the vagina.
- Deep margin – This is the tissue inside the wall of the cervix.
- Radial margin – This is the soft tissue that surrounds the cervix. The radial margin will only be described in your report if you had your entire cervix and uterus removed at the same time.
What information is used to determine the pathologic stage for adenocarcinoma of the cervix?
The pathologic stage for adenocarcinoma of the cervix is based on the TNM staging system, an internationally recognized system originally created by the American Joint Committee on Cancer. This system uses information about the primary tumour (T), lymph nodes (N), and distant metastatic disease (M) to determine the complete pathologic stage (pTNM). Your pathologist will examine the tissue submitted and give each part a number. In general, a higher number means a more advanced disease and a worse prognosis.
Tumour stage (pT) for adenocarcinoma of the cervix
The pathologic tumour stage for adenocarcinoma of the cervix is based on three factors: the amount of stromal invasion, the size of the tumour, and the extension of the tumour into surrounding organs or tissues.
- T1a – Tumours in this category were found only after the tissue was examined under the microscope. These tumours also have a depth of invasion that is 5 millimetres or less AND and a horizontal spread that is 7 millimetres or less.
- T1b – Your doctor saw the tumour during your physical examination OR the depth of invasion is greater than 5 millimetres OR the horizontal spread is greater than 7 millimetres.
- T2a – The tumour extends outside of the uterus but not into the parametrium.
- T2b – The tumour extends into the parametrium.
- T3a – The tumour extends to the lower part of the vagina.
- T3b – The tumour extends into the wall of the pelvis OR the tumour has caused injury to the kidney.
- T4 – The tumour extends into the bladder or rectum OR the tumour extends outside of the pelvis into the abdomen.
Nodal stage (pN) for adenocarcinoma of the cervix
The pathologic nodal stage (pN) is based on the examination of lymph nodes for cancer cells.
- NX – No lymph nodes were sent to pathology for examination.
- N0 – No cancer cells were found in any of the lymph nodes examined.
- N0(i+) – Only isolated cancer cells were found in a lymph node.
- N1 – A group of cancer cells larger than 0.2 millimetres was found in at least one lymph node.
Metastatic stage (pM) for adenocarcinoma of the cervix
Adenocarcinoma of the cervix is given a metastatic stage of 0 or 1 based on the presence of cancer cells at a distant site in the body (for example the lungs). The metastatic stage can only be assigned if tissue from a distant site is submitted for pathological examination. Because this tissue is rarely present, the metastatic stage cannot be determined and is listed as MX.
About this article
This article was written by doctors to help you read and understand your pathology report. Contact us if you have any questions about this article or your pathology report. Read this article for a more general introduction to the parts of a typical pathology report.
Other helpful resources
Atlas of Pathology
We are proud to partner with:
![]()