

by Jason Wasserman MD PhD FRCPC
December 2, 2024
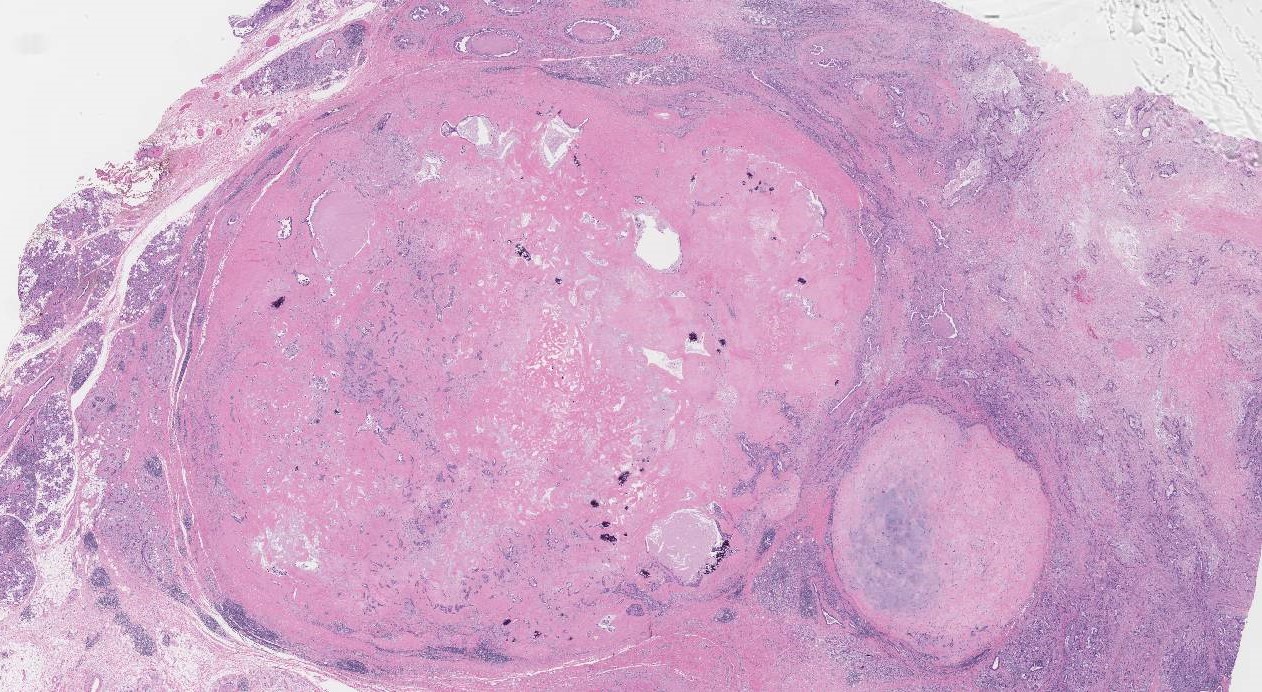
Carcinoma ex pleomorphic adenoma is a type of salivary gland cancer that develops from within a previously benign (noncancerous) tumour called pleomorphic adenoma. In pathology, carcinoma is a general term used to describe a group of malignant (cancerous) tumours made up of epithelial cells, while “ex” means “out of” or “from”. Put together, carcinoma ex pleomorphic adenoma is a malignant tumour made up of epithelial cells developing from a pleomorphic adenoma. Most carcinoma ex pleomorphic adenomas are found in the parotid gland. However, any of the salivary glands, including the minor salivary glands in the oral cavity, can be involved.

What are the symptoms of carcinoma ex pleomorphic adenoma?
The most common symptom of carcinoma ex pleomorphic adenoma is the sudden growth of a tumour that has been present for many months or years. Additional symptoms include pain and weakness in the area of the tumour.
What causes carcinoma ex pleomorphic adenoma?
Carcinoma ex pleomorphic adenoma arises from a preexisting pleomorphic adenoma. We do not know why some pleomorphic adenomas undergo this change while others do not.
What are the most common types of cancerous tumours that develop from within a pleomorphic adenoma?
Any type of salivary gland cancer can develop from within a pleomorphic adenoma. However, the most common types of cancers associated with pleomorphic adenoma are:
- Salivary duct carcinoma ex pleomorphic adenoma: Salivary duct carcinoma is an aggressive type of salivary gland cancer and the most common type of cancer to develop from within a pleomorphic adenoma. It frequently spreads to lymph nodes and other parts of the body.
- Myoepithelial carcinoma ex pleomorphic adenoma: Myoepithelial carcinoma is a type of salivary gland cancer made up entirely of myoepithelial cells. It can spread to lymph nodes and other body parts, such as the lungs.
- Adenocarcinoma, NOS ex pleomorphic adenoma: Adenocarcinoma, NOS is a type of salivary gland cancer made up of cells that do not show features of any other type of salivary gland cancer. The behaviour of this type of cancer is variable.
Invasive versus noninvasive tumours
When examining a carcinoma ex pleomorphic adenoma, pathologists look to see whether the carcinoma is entirely inside the capsule (boundary) of the original benign pleomorphic adenoma or if it has spread through the capsule into the surrounding tissue. Tumours that have spread through the capsule are called invasive, while those that have not are called noninvasive. This spread is an important factor in determining the tumour’s behaviour and prognosis.
- Intracapsular: This is another term used to describe a noninvasive tumour. The cancer cells have not broken through the capsule; thus, the tumour is contained. Intracapsular tumours are associated with a good prognosis.
- In situ: In situ refers to cancer cells that are found within spaces called ducts. This is an early stage of cancer where the cells have not spread into the surrounding tissues. As such, it is usually associated with a good prognosis.
- Minimally invasive: This indicates that the carcinoma has begun to invade surrounding tissues but to a very limited extent. The invasion is usually defined by a specific measurement, often less than 1.5 millimetres beyond the capsule. The prognosis for a patient with a minimally invasive tumour depends on the carcinoma type but is usually better than a widely invasive tumour.
- Widely invasive: Widely invasive means the carcinoma has extensively spread into surrounding tissues beyond the original tumour site. This extensive invasion indicates a more aggressive tumour and often correlates with a worse prognosis.
What does it mean if my report says the tumour is intracapsular?
Carcinoma ex pleomorphic adenoma is described as intracapsular when all of the malignant (cancerous) cells are found within the capsule (border) of the previously benign (noncancerous) pleomorphic adenoma. Intracapsular means that the cancerous cells have not yet spread into the surrounding tissue. Compared with minimally invasive and invasive tumours (see below), intracapsular tumours are less likely to spread to lymph nodes or other body parts and are typically cured by surgery alone.
What does it mean if my report says the tumour is in situ?
Carcinoma ex pleomorphic adenoma is described as in situ if all of the malignant (cancerous) cells are found within round structures called ducts, and the ducts are located entirely within the capsule (border) of the previously benign (noncancerous) pleomorphic adenoma. Another term used to describe an in situ tumour is non-invasive. Compared with minimally invasive and invasive tumours (see below), in situ tumours are less likely to spread to lymph nodes or other body parts and are typically cured by surgery alone.
What does it mean if my report says the tumour is minimally invasive?
Carcinoma ex pleomorphic adenoma is described as minimally invasive when the malignant (cancerous) cells have spread no more than 4 to 6 mm past the capsule (border) of the previously benign (noncancerous) pleomorphic adenoma and into the surrounding tissue. Compared with invasive tumours (see below), minimally invasive tumours are associated with better overall prognosis.
What does it mean if my report says the tumour is invasive?
Carcinoma ex pleomorphic adenoma is described as invasive when the malignant (cancerous) cells have spread more than 6 mm past the capsule (border) of the previously benign (noncancerous) pleomorphic adenoma and into the surrounding tissue. Compared with intracapsular and minimally invasive tumours (see above), invasive tumours are more likely to spread to lymph nodes and are associated with a worse overall prognosis.
Perineural invasion
Perineural invasion (PNI) is the process by which cancer cells spread along or around nerves. This phenomenon is significant in head and neck cancers, including carcinoma ex pleomorphic adenoma. Cancer cells can travel along the nerve fibres to reach areas beyond the primary tumour site when they invade the perineural spaces. Perineural invasion is an important pathological feature because it can indicate a higher risk of local recurrence and can be associated with a more aggressive disease course. Symptoms related to perineural invasion may include pain or nerve dysfunction, depending on the nerves involved.

Lymphovascular invasion
Lymphovascular invasion (LVI) refers to the presence of cancer cells within the lymphatic system or blood vessels. This type of invasion is a critical step in the metastatic spread of cancer, as it allows tumour cells to travel through the lymphatic system or bloodstream to distant sites in the body. In carcinoma ex pleomorphic adenoma, lymphovascular invasion is important in determining the prognosis and guiding treatment decisions. The presence of lymphovascular invasion typically suggests a higher likelihood of metastasis, particularly to regional lymph nodes or other organs, which can affect the overall treatment approach and outcome.

Margins
In pathology, a margin is the edge of tissue removed during tumour surgery. The margin status in a pathology report is important as it indicates whether the entire tumour was removed or if some was left behind. This information helps determine the need for further treatment.
Pathologists typically assess margins following a surgical procedure, like an excision or resection, that removes the entire tumour. Margins aren’t usually evaluated after a biopsy, which removes only part of the tumour. The number of margins reported and their size—how much normal tissue is between the tumour and the cut edge—vary based on the tissue type and tumour location.
Pathologists examine margins to check if tumour cells are present at the tissue’s cut edge. A positive margin, where tumour cells are found, suggests that some cancer may remain in the body. In contrast, a negative margin, with no tumour cells at the edge, suggests the tumour was fully removed. Some reports also measure the distance between the nearest tumour cells and the margin, even if all margins are negative.

Lymph nodes
Small immune organs, known as lymph nodes, are located throughout the body. Cancer cells can travel from a tumour to these lymph nodes via tiny lymphatic vessels. For this reason, doctors often remove and microscopically examine lymph nodes to look for cancer cells. This process, where cancer cells move from the original tumour to another body part, like a lymph node, is termed metastasis.
Cancer cells usually first migrate to lymph nodes near the tumour, although distant lymph nodes may also be affected. Consequently, surgeons typically remove lymph nodes closest to the tumour first. They might remove lymph nodes farther from the tumour if they are enlarged and there’s a strong suspicion they contain cancer cells.

Pathologists will examine any removed lymph nodes under a microscope; the findings will be detailed in your report. A “positive” result indicates the presence of cancer cells in the lymph node, while a “negative” result means no cancer cells were found. If the report finds cancer cells in a lymph node, it might also specify the size of the largest cluster of these cells, often referred to as a “focus” or “deposit.” Extranodal extension occurs when tumour cells penetrate the lymph node’s outer capsule and spread into the adjacent tissue.
Examining lymph nodes is important for two reasons. First, it helps determine the pathologic nodal stage (pN). Second, discovering cancer cells in a lymph node suggests an increased risk of later finding cancer cells in other body parts. This information guides your doctor in deciding whether you need additional treatments, such as chemotherapy, radiation therapy, or immunotherapy.
We are proud to partner with:
![]()