

by Jason Wasserman MD PhD FRCPC and Zuzanna Gorski MD FRCPC
May 14, 2026
Cervical intraepithelial neoplasia (CIN) is a precancerous condition of the cervix caused by infection with human papillomavirus (HPV). It is composed of squamous cells infected and altered by the virus. These abnormal cells are found in the transformation zone — the part of the cervix where glandular cells are gradually replaced by squamous cells. CIN is not cancer, but it is called precancerous because, if untreated, it can progress over time to cervical cancer, most often HPV-associated squamous cell carcinoma. CIN is divided into three levels based on how much of the surface lining of the cervix has been replaced by abnormal cells: CIN1, CIN2, and CIN3. The risk of progression to cancer is lowest with CIN1 and highest with CIN3. This article will help you understand the findings in your pathology report — what each term means and why it matters for your care.
What causes cervical intraepithelial neoplasia?
CIN is caused by persistent infection with high-risk types of HPV — most commonly HPV16 and HPV18, with HPV31, 33, 45, 52, and 58 contributing additional cases. HPV is a very common virus that spreads through sexual contact. Most HPV infections, including high-risk types, clear on their own within one to two years as the immune system eliminates the virus. Only a small percentage of infections persist in the cervix, and these long-lasting infections can lead to CIN.
When a high-risk HPV infection persists, the virus produces proteins that interfere with the systems that normally control cell growth. Over months to years, this can cause the squamous cells of the cervix to grow abnormally — first in the deepest layer of the lining, then progressively higher as the disease advances from CIN1 to CIN3. Higher-grade CIN (CIN2 and CIN3) usually develops only after a persistent infection lasting 2 years or more. This slow progression is the reason regular Pap tests and HPV testing are so effective at preventing cervical cancer: there is a long window of time during which precancerous changes can be found and treated before they progress.
What are the symptoms?
CIN almost never causes symptoms. The cells affected by CIN remain confined to the surface lining of the cervix and do not invade deeper tissue, so they do not produce bleeding, pain, or discharge in most people. For this reason, CIN is almost always discovered through cervical cancer screening rather than because of symptoms. Regular Pap tests and HPV testing remain the most reliable way to find CIN before it has a chance to progress.
How is the diagnosis made?
The diagnosis of CIN is made by examining cells or tissue from the cervix under the microscope. The process usually begins with an abnormal Pap test or a positive HPV test, which then leads to a closer evaluation called colposcopy. During colposcopy, the doctor uses a colposcope — a special magnifying instrument — to examine the surface of the cervix in detail. Any area that looks abnormal is sampled with a biopsy: a small piece of tissue is removed and sent to the pathology laboratory. In some cases, a sample is also collected from inside the cervical canal using a procedure called endocervical curettage, particularly when the area of concern may extend into the canal, where it cannot be fully seen with the colposcope.
If a biopsy confirms CIN — particularly the higher-grade forms — or if a more complete assessment is needed, a larger tissue removal procedure is often performed. The two most common options are a loop electrosurgical excision procedure (LEEP), in which a thin wire loop heated by an electric current removes a layer of cervical tissue, and a cone biopsy (also called conization), in which a cone-shaped portion of the cervix is removed. Both procedures include the transformation zone and provide more tissue for the pathologist to examine.
Under the microscope, the pathologist looks at how much of the epithelium (the surface lining of the cervix) has been replaced by abnormal squamous cells. The depth and severity of the abnormal change determine the grade of CIN. To support the diagnosis, especially for higher-grade CIN, a special protein stain called p16 is often performed. Cells infected with high-risk HPV produce large amounts of p16, so strong and continuous staining for this protein supports a diagnosis of CIN2 or CIN3 and helps distinguish these lesions from non-HPV-related conditions that can look similar. CIN1 is usually negative or only weakly positive for p16.
Grading of cervical intraepithelial neoplasia
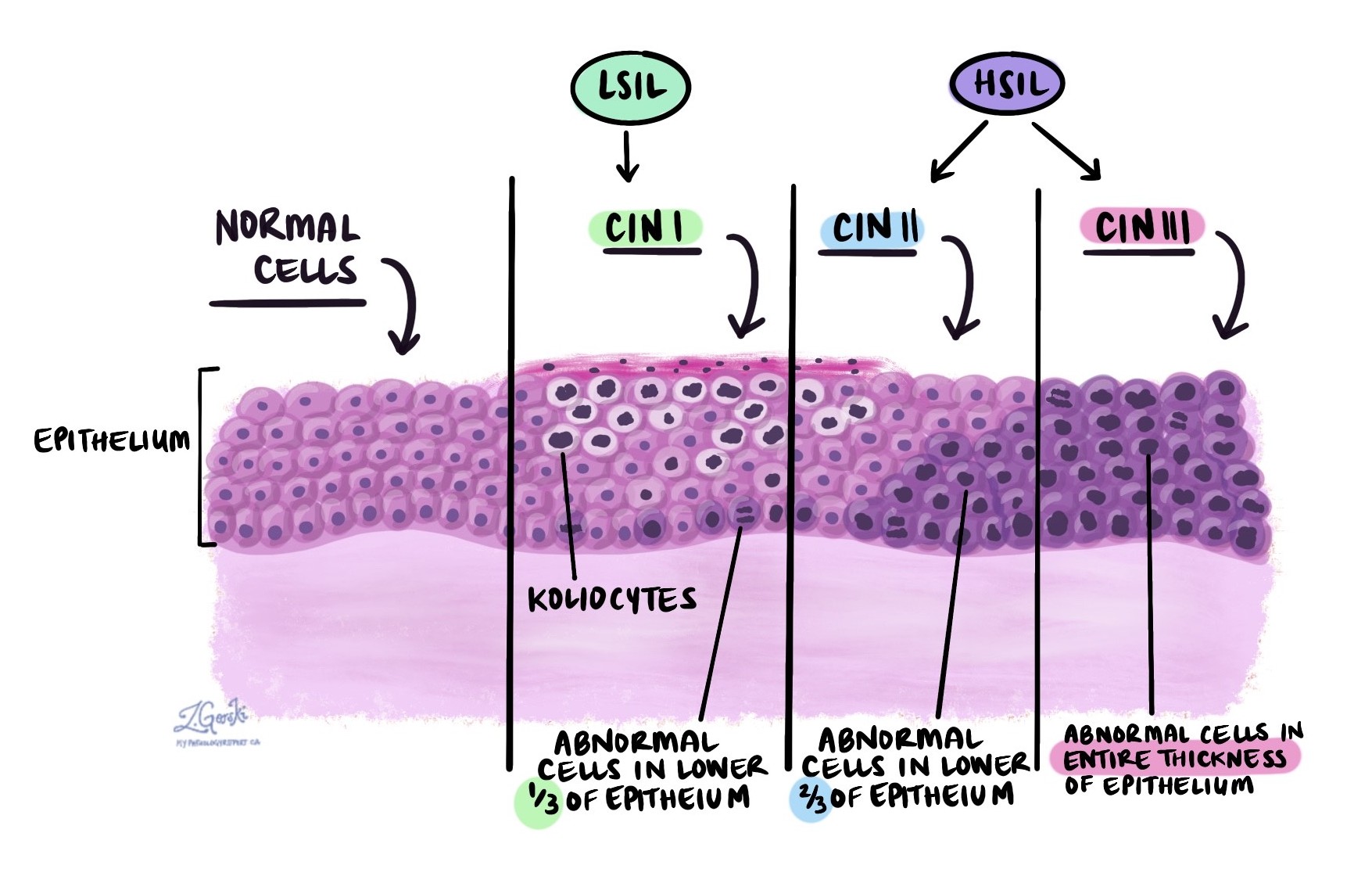
The grade of CIN describes how much of the cervical epithelium has been replaced by abnormal squamous cells. The grade is important because it predicts the risk of progression to cervical cancer and guides treatment decisions. Three grades are used:
- CIN1 (also called low-grade squamous intraepithelial lesion, LSIL) — Abnormal squamous cells are confined to the lower one-third of the epithelium. A hallmark feature is the presence of koilocytes, which are squamous cells infected by HPV. Koilocytes are larger than normal, have irregular dark nuclei, and often show a clear space (or “halo”) around the nucleus. Some koilocytes have more than one nucleus. The pathologist may also see an increased number of mitotic figures (dividing cells). The risk of CIN1 progressing to cancer is low, and in most people, CIN1 resolves on its own without treatment.
- CIN2 (also called high-grade squamous intraepithelial lesion, HSIL) — Abnormal cells are found in the lower two-thirds of the epithelium. The cells are darker than normal (a feature called hyperchromatic), immature, and lack the normal maturation that squamous cells usually develop as they move toward the surface. The cells have less cytoplasm compared to their nuclei, making the overall appearance darker. Dividing cells are more numerous, and some show abnormal division patterns called atypical mitotic figures. CIN2 carries a higher risk of progression to cancer than CIN1.
- CIN3 (also called high-grade squamous intraepithelial lesion, HSIL) — Abnormal squamous cells are seen throughout the entire thickness of the epithelium, from the surface to the base. The cells are dark, immature, and have very little cytoplasm relative to their nuclei. Many dividing cells, including atypical mitotic figures, are seen. CIN3 carries the highest risk of progressing to cervical cancer, and treatment is almost always recommended to remove the abnormal tissue.
Because CIN2 and CIN3 are both categorized as HSIL and are managed in a similar way, your pathology report may use the terms HSIL and CIN2 or CIN3 together. CIN1, by contrast, is the same as LSIL and is managed quite differently from the higher-grade lesions.
Surgical margins
A margin is the cut edge of tissue that was removed during a surgical procedure, such as a LEEP or cone biopsy. After surgery, the pathologist examines the margins under the microscope to determine whether any CIN cells are present at the cut edge. Margins are reported only in excision specimens — not in Pap tests or small biopsies, which are not intended to remove the entire lesion.
- Negative margin — No CIN is present at the cut edge of the tissue. This is the most reassuring result and suggests the abnormal area was completely removed.
- Positive margin — CIN is present at the cut edge. This means some abnormal cells may remain in the cervix, increasing the risk that CIN could recur. Repeat surgery or closer follow-up is typically recommended.
Three margin locations are assessed in cervical excision specimens:
- Endocervical margin — The inner edge of the specimen, closest to the uterus. Involvement of this margin is particularly important because abnormal cells may remain high in the endocervical canal, where they are difficult to detect on follow-up screening.
- Ectocervical margin — The outer edge of the specimen, closest to the vagina.
- Stromal margin — The deep edge, corresponding to the wall of the cervix beneath the removed tissue.
What is the prognosis?
CIN is considered a precancerous condition because it has the potential to progress to cervical cancer if not treated. However, the risk of progression depends strongly on the grade and on whether the underlying HPV infection persists. With regular screening and appropriate treatment, CIN is almost always detected and managed before it has the chance to become cancer.
- CIN1 — The risk of progression to cancer is low. Most cases (approximately 60%) resolve on their own within two years, especially in younger people whose immune system clears the underlying HPV infection. For this reason, observation with repeat Pap and HPV testing is usually preferred over immediate treatment.
- CIN2 — The risk of progression to cancer is moderate. Approximately 40% of CIN2 lesions resolve spontaneously, particularly in younger people, whereas the remainder persist or progress without treatment. Management depends on age, fertility considerations, and the appearance of the lesion.
- CIN3 — The risk of progression to cancer is high. Without treatment, a meaningful proportion of CIN3 lesions progress to invasive cervical cancer over many years. Because of this risk, treatment is almost always recommended once CIN3 is confirmed.
- Persistent HPV infection — Across all grades, persistence of high-risk HPV infection is the most important risk factor for both progression and recurrence. Clearance of HPV after treatment is a strong predictor of cure.
- Margin status after excision — Negative margins after a LEEP or cone biopsy carry a low risk of recurrence. Positive margins, especially when located at the endocervical edge, increase the risk of residual disease and may require further treatment.
What happens after this diagnosis?
Treatment recommendations for CIN depend on the grade, your age, whether you wish to preserve fertility, the size and location of the lesion, and your HPV test results.
For CIN1, treatment is usually not required immediately. The standard approach is observation with repeat Pap testing or HPV testing in 6 to 12 months, which allows time for the immune system to clear the underlying HPV infection. If CIN1 persists for two years or more, treatment may be considered.
For CIN2, management is more individualized. In younger people who wish to preserve fertility — particularly those under 25 — close observation may be offered because of the higher rate of natural resolution. In other situations, or if the lesion persists, treatment with a LEEP or cone biopsy is recommended to remove the abnormal area before it progresses.
For CIN3, treatment is almost always recommended. A LEEP or cone biopsy is the standard approach for most patients. Hysterectomy (surgical removal of the uterus and cervix) is generally not required for CIN3 but may be considered in specific situations, such as recurrent CIN3 after multiple excisions or when other gynecologic conditions are also present.
After treatment, regular follow-up is essential. The standard schedule includes Pap testing and HPV testing 6 months after treatment, followed by additional testing at 12 and 24 months. After two consecutive negative test results, most people can return to routine screening intervals. Your doctor or gynecologic specialist will tailor the follow-up plan based on your treatment, margin status, HPV results, and overall medical history.
Questions to ask your doctor
- What grade of CIN was found in my biopsy — CIN1, CIN2, or CIN3?
- Was p16 staining performed on my biopsy, and what did the result show?
- Did my sample test positive for high-risk HPV, and which type?
- Do I need treatment now, or is observation a safe option for my situation?
- If treatment is recommended, what are my options — LEEP, cone biopsy, or something else?
- I want to preserve my fertility — is conservative management appropriate for me?
- Were the margins clear after my procedure, and what does the margin status mean for my next steps?
- What is my risk of CIN coming back or progressing to cancer?
- How often will I need follow-up Pap tests or HPV testing, and for how long?
- When can I return to routine cervical cancer screening?
- Should I consider HPV vaccination if I have not already been vaccinated?
- What symptoms should prompt me to contact you between scheduled appointments?
Related articles on MyPathologyReport.com
- Low grade squamous intraepithelial lesion (LSIL) of the cervix
- High grade squamous intraepithelial lesion (HSIL) of the cervix
- HPV-associated squamous cell carcinoma of the cervix
- HPV-independent squamous cell carcinoma of the cervix
- Adenocarcinoma in situ (AIS) of the cervix
- ASC-US of the cervix
- ASC-H of the cervix
- Negative for intraepithelial lesion or malignancy (NILM)
- Pap test
- Human papillomavirus (HPV)
- High-risk HPV
- p16
We are proud to partner with:
![]()