

by Bibianna Purgina, MD FRCPC
September 3, 2022
Chordoma is a type of bone cancer. It develops from remnants of an embryonic structure called the notochord. Chordomas almost always develop within a bone and most develop along the midline of the body in either the base of the skull or the sacrum. Chordomas are very slow-growing tumours and can reach a very large size, especially those that develop around the pelvis.
What type of cancer is a chordoma?
Chordoma is a type of sarcoma. Sarcomas are cancers that start from mesenchymal tissues such as bone, cartilage, muscle, and nerves.
How do chordomas start?
Chordomas develop from cells left over from an embryonic structure called the notochord. The notochord helps to form the bones in the spine during fetal development. Once the spine has formed, the cells of the notochord usually disappear. Sometimes small areas of notochord cells remain and it is from these leftover cells (called remnants) that chordoma develops.
The two most common locations are the sacrum (the bottom of the spine in the pelvis) and the base of the skull. Very rarely chordoma can develop in a non-bone location away from the midline of the body. Most chordomas occur in older patients, usually between the ages of 40 to 70 although they can occur in younger patients including children.
What are the symptoms of chordoma?
Symptoms related to chordoma depend on the location of the tumour. Chordomas that develop in the skull base can cause headaches or vision problems. Those that develop in the pelvis can cause bladder or bowel problems or tingling in the legs.
How is chordoma diagnosed?
The first diagnosis of a chordoma is usually made after a small piece of the tumour is removed in a procedure called a biopsy. The tissue is then sent to a pathologist for examination under the microscope. After a pathologist makes a diagnosis of chordoma, most patients undergo surgery to remove the tumour although some patients may be offered radiation therapy before surgery. Chordoma is a type of cancer that usually does not respond to chemotherapy.
What does chordoma look like under the microscope?
Under the microscope, chordomas are made of round to oval-shaped tumour cells. Some of the tumour cells will have small holes inside of the cells which pathologists describe as vacuoles. The tumour cells with vacuoles are called physaliferous cells.

About this article
This article was written by doctors to help you read and understand your pathology report for chordoma. The sections below describe the results found in most pathology reports, however, all reports are different and results may vary. Importantly, some of this information will only be described in your report after the entire tumour has been surgically removed and examined by a pathologist. Contact us if you have any questions about this article or your pathology report. Read this article for a more general introduction to the parts of a typical pathology report.
What are the histologic types of chordoma?
There are different types of chordoma and each one is called a histologic type. The histologic type is based on the way the tumour looks when examined under the microscope. The histologic type of chordoma is important because it is used to determine the grade (see Grade below).
The histologic types of chordoma include:
- Conventional chordoma – The tumour cells look like they are floating in a blue or grey called material that pathologists describe as myxoid or mucinous.
- Chondroid chordoma – The tumour cells are surrounded by a material that looks like cartilage.
- Cellular chordoma – Most of the tumour is made up of large groups of tumour cells with very little material in the background.
- Poorly differentiated chordoma – The tumour cells look very abnormal compared to the other types of chordoma and there are no physaliferous cells.
- Dedifferentiated chordoma – Some chordomas will change over time so that some of the cells no longer resemble normal chordoma cells. This process is called dedifferentiation and these chordomas are then called dedifferentiated chordomas.
How do pathologists grade chordoma and why is the grade imporant?
Grade is a word pathologists use to describe how different the tumour looks compared to the normal cells in the bone. Bone tumours are graded on a scale of 1 to 3 with grade 1 tumours considered ‘low grade’ while grade 3 tumours are considered ‘high grade’. For most bone tumors, the grade is determined by the histologic type of the tumour. Conventional, cellular, and chondroid chordomas are grade 2 (intermediate grade), but poorly differentiated and dedifferentiated chordomas are grade 3 (high grade).
The grade is important because it is used to predict the behavior of the tumour. For example, grade 1 tumours may come back in the same location (local recurrence) but it is rare for them to spread to more distant parts of the body. Higher grade tumours (grades 2 and 3) are more likely to spread to distant parts of the body and are usually associated with a worse prognosis.
Has the tumour spread into surrounding tissues?
Large chordomas often break through the bone and grow into the surrounding tissue including adjacent organs, muscles, tendons, or the joint space. If this has occurred, it may be included in your report and is usually described as extraosseous extension. Some bones are made up of multiple parts. If the chordoma has grown from one part into another, your report will describe the tumour as invading adjacent bones. This is particularly important for tumours in the spine or pelvis as both bones are made up of multiple parts.
What does treatment effect mean?
If you have been diagnosed with chordoma on a biopsy, you usually will have surgery first to remove the tumour. In some cases of chordoma, pre-surgery radiation therapy may be given. If you have received radiation therapy before your surgery, your pathologist will examine all the tissue sent to pathology to see how much of the tumour is still viable (alive).
What does perineural invasion mean and why is it important?
The presence of cancer cells wrapped around a nerve is called perineural invasion. Perineural invasion is important because cancer cells can travel along a nerve to tissues far away from the original tumour. Perineural invasion is not commonly seen in chordoma.

What does lymphovascular invasion mean and why is it important?
Lymphatics and blood vessels are channels that normal cells use to travel around the body. The presence of cancer cells within a lymphatic or blood vessel is called lymphovascular invasion and is associated with a higher risk that the cancer cells will travel to a distant site such as the lungs. Chordomas rarely metastasize to lymph nodes.

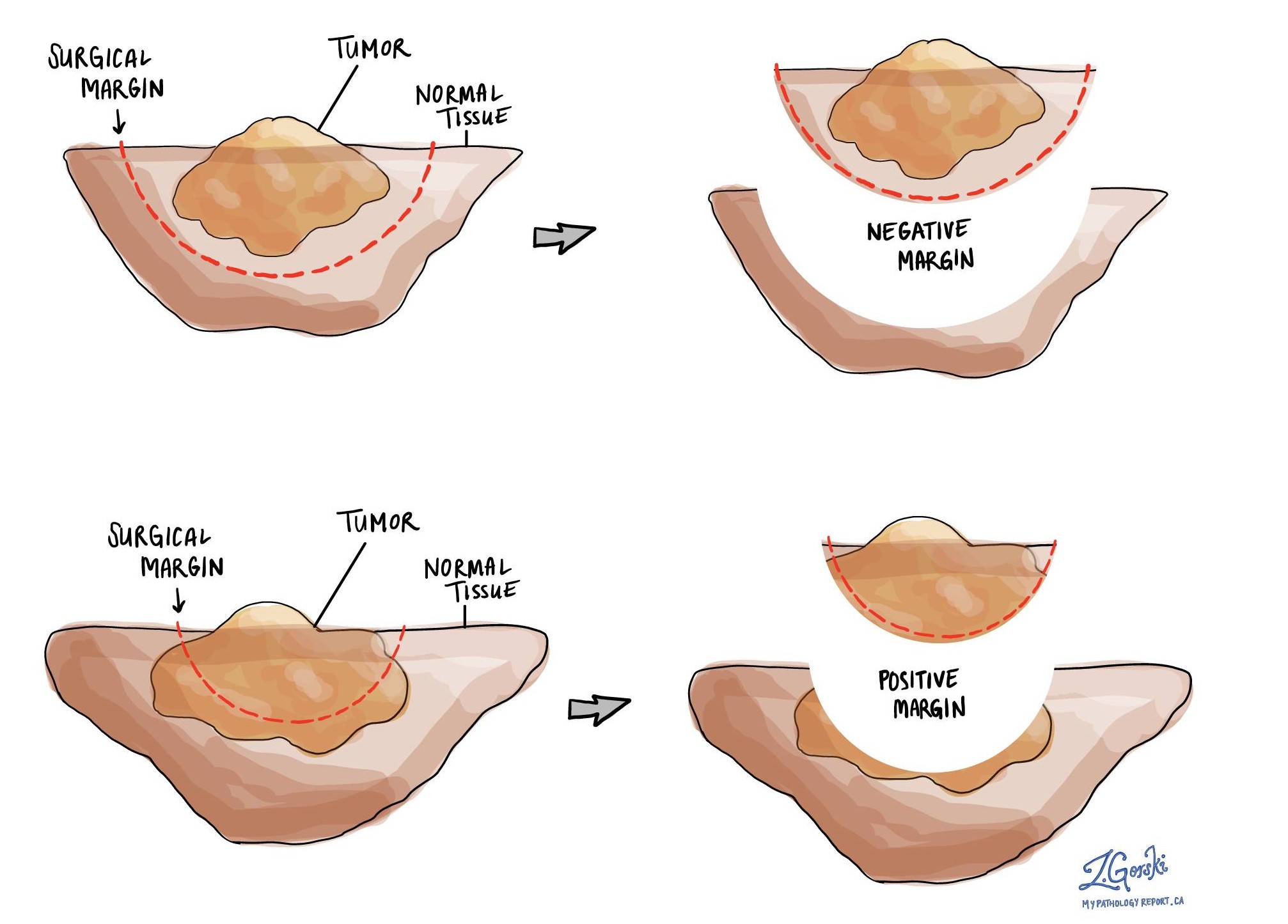
What is a margin and why are margins important?
A margin is any tissue that was cut by the surgeon to remove the bone (or part of the bone) and tumour from your body. Depending on the type of surgery you have had, the types of margins, which could include proximal (the part of the bone closest to the middle of your body) and distal (the part of the bone farthest from the middle of your body) bone margins, soft tissue margins, blood vessel margins, and nerve margins.
All margins will be very closely examined under the microscope by your pathologist to determine the margin status. A margin is considered negative when there are no cancer cells at the edge of the cut tissue. A margin is considered positive when there are cancer cells at the edge of the cut tissue. A positive margin is associated with a higher risk that the tumour will recur in the same site after treatment (local recurrence).
Chordomas that occur in the skull base are often taken out as multiple small pieces which make it impossible for the pathologist to examine the margins of the tissue. In this situation, the completeness of the surgery will be determined by the radiologist using post-operative imaging such as CT scans or MRI scans.
What are lymph nodes and why are they important?
Lymph nodes are small immune organs found throughout the body. Cancer cells can spread from a tumour to lymph nodes through small vessels called lymphatics. The cancer cells in chondroblastic osteosarcoma typically do not spread to lymph nodes and for this reason, lymph nodes are not always removed at the same time as the tumour. However, when lymph nodes are removed, they will be examined under a microscope and the results will be described in your report.

Cancer cells typically spread first to lymph nodes close to the tumour although lymph nodes far away from the tumour can also be involved. For this reason, the first lymph nodes removed are usually close to the tumour. Lymph nodes further away from the tumour are only typically removed if they are enlarged and there is a high clinical suspicion that there may be cancer cells in the lymph node. Most reports will include the total number of lymph nodes examined, where in the body the lymph nodes were found, and the number (if any) that contain cancer cells. If cancer cells were seen in a lymph node, the size of the largest group of cancer cells (often described as “focus” or “deposit”) will also be included.
The examination of lymph nodes is important for two reasons. First, this information is used to determine the pathologic nodal stage (pN). Second, finding cancer cells in a lymph node increases the risk that cancer cells will be found in other parts of the body in the future. As a result, your doctor will use this information when deciding if additional treatment such as chemotherapy, radiation therapy, or immunotherapy is required.
What does it mean if a lymph node is described as positive?
Pathologists often use the term “positive” to describe a lymph node that contains cancer cells. For example, a lymph node that contains cancer cells may be called “positive for malignancy”.
What does it mean if a lymph node is described as negative?
Pathologists often use the term “negative” to describe a lymph node that does not contain any cancer cells. For example, a lymph node that does not contain cancer cells may be called “negative for malignancy”.
What is the pathologic stage for chordoma?
The pathologic stage for chordoma is based on the TNM staging system, an internationally recognized system originally created by the American Joint Committee on Cancer. This system uses information about the primary tumour (T), lymph nodes (N), and distant metastatic disease (M) to determine the complete pathologic stage (pTNM). Your pathologist will examine the tissue submitted and give each part a number. In general, a higher number means more advanced disease and a worse prognosis.
Tumour stage (pT)
For bone cancers such as chordoma, the primary tumour (pT) stage depends on where the tumour was located in your body. If the chordoma was located in your appendicular skeleton (specifically the bones of the skull), it is given a tumour stage from 1-3 based on tumour size and whether there is a separate tumor nodule(s).
- pT1: Tumor ≤ 8 cm in greatest dimension.
- pT2: Tumor > 8 cm in greatest dimension.
- pT3: Discontinuous tumors in the primary bone site.
If the chordoma was located in your spine, it is given a tumour stage from 1-4 based on the extent of tumor growth.
- pT1: Tumor confined to one vertebral segment or two adjacent vertebral segments.
- pT2: Tumor confined to three adjacent vertebral segments.
- pT3: Tumor confined to four or more adjacent vertebral segments, or any nonadjacent vertebral segments.
- pT4: Extension into the spinal canal or great vessels.
If the chordoma was located in your pelvis, it is given a tumour stage from 1-4 based on the size of the tumour and the extent of tumor growth.
- pT1: Tumor confined to one pelvic segment with no extraosseous (growing outside of the bone) extension.
- pT1a: Tumor ≤ 8 cm in greatest dimension.
- pT1b: Tumor >8 cm in greatest dimension.
- pT2: Tumor confined to one pelvic segment with extraosseous extension or two segments without extraosseous extension.
- pT2a: Tumor ≤ 8 cm in greatest dimension.
- pT2b: Tumor >8 cm in greatest dimension.
- pT3: Tumor spanning two pelvic segments with extraosseous extension.
- pT3a: Tumor ≤ 8 cm in greatest dimension.
- pT3b: Tumor >8 cm in greatest dimension.
- pT4: Tumor spanning three pelvic segments or crossing the sacroiliac joint.
- pT4a: Tumor involves sacroiliac joint and extends medially to the sacral neuroforamen (space where the nerves pass through).
- pT4b: Tumor encasement of external iliac vessels or presence of gross tumor thrombus in major pelvic vessel.
If your pathologist cannot reliably evaluate the tumor size or the extent of growth, it is given the tumour stage pTX (primary tumour cannot be assessed). This may happen if the tumour is received as multiple small fragments.
Nodal stage (pN)
Primary bone cancers are given a nodal stage of 0 or 1 based on the presence or absence of cancer cells in one or more lymph nodes. If no cancer cells are seen in any lymph nodes, the nodal stage is N0. If no lymph nodes are sent for pathological examination, the nodal stage cannot be determined, and the nodal stage is listed as NX. If cancer cells are found in any lymph nodes, then the nodal stage is listed as N1.
Metastasis stage (pM)
Bone sarcomas are given a metastasis stage only if the presence of metastasis has been confirmed by a pathologist. There are two metastasis stages in primary bone sarcomas, M1a and M1b. If there are confirmed lung metastasis, then the tumor metastasis stage is 1a. The metastasis stage can only be given if tissue from a distant site is sent for pathological examination. Because this tissue is rarely present, the metastasis stage cannot be determined, and it is typically not included in your report.
Other helpful resources
Atlas of Pathology
We are proud to partner with:
![]()