

by Jason Wasserman MD PhD FRCPC and Trevor Flood MD FRCPC
August 29, 2022
What is HPV-associated squamous cell carcinoma of the penis?
HPV-associated squamous cell carcinoma (SCC) is a type of cancer that starts from the cells on the surface of the penis. It is a sexually transmitted disease.
What causes HPV-associated squamous cell carcinoma of the penis?
As its name suggests, HPV-associated SCC is caused by a virus called human papillomavirus (HPV). HPV is a sexually transmitted virus that is very common among adults. The virus infects cells on the surface of the penis. Over time, the virus causes changes inside the infected cells that lead to the development of cancer.
How is the diagnosis of HPV-associated squamous cell carcinoma of the penis made?
The diagnosis of HPV-associated SCC of the penis is usually made after a small piece of tissue is removed in a procedure called a biopsy. The tissue is then sent to a pathologist for examination under the microscope. After the diagnosis is made, your doctor may recommend removing the entire tumour. If removed, the tumour will also be sent to a pathologist for examination under the microscope.
What are the types of HPV-associated squamous cell carcinoma of the penis?
The four most common types of HPV-associated SCC of the penis are basaloid, warty, clear cell, and lymphoepithelioma-like. The tumour type can only be determined after the tumour is examined under the microscope by a pathologist. The basaloid and clear cell types are aggressive cancers that frequently spread to lymph nodes in the inguinal canal and pelvis. In contrast, the warty type is considered a less aggressive cancer that can spread to lymph nodes but at a lower rate than the basaloid or clear cell types.
What does it mean if the tumour is described as invasive?
HPV-associated SCC of the penis starts from squamous cells that are found in the skin on the surface of the penis. Invasive means that the cancer cells have spread into the tissue below the skin. Your pathologist must see invasion in order to make the diagnosis of SCC. When the abnormal cells are only found in the skin, the disease is called penile intraepithelial neoplasia (PeIN).
What is penile intraepithelial neoplasia (PeIN)?
Penile intraepithelial neoplasia (PeIN) is a non-invasive precancerous disease that involves the penis. It is called “non-invasive” because the abnormal cells are only found in the skin on the surface of the penis. If left untreated, PeIN can turn into SCC over time.
What does it mean if the tumour is positive for p16?
p16 is a protein that is produced by both normal cells and cancer cells. Pathologists perform a special test called immunohistochemistry in order to be able to see p16 protein inside cells. Tumours caused by HPV produce extra p16 which builds up inside the cancer cells. For this reason, the cancer cells in most HPV-associated SCCs of the penis and scrotum will make extra p16. Your pathology report will describe these cells as positive for p16.
What does it mean if the tumour is described as keratinizing?
HPV-associated SCC of the penis and scrotum is described as “keratinizing” if the cancer cells produce large amounts of a specialized protein called keratin. When examined under the microscope, cancer cells that produce large amounts of keratin appear pink. In contrast, the cancer cells in a non-keratinizing tumour look blue.
How is HPV-associated squamous cell carcinoma of the penis graded?
Pathologists use the term differentiated to divide HPV-associated squamous cell carcinoma of the penis into three grades – well-differentiated, moderately differentiated, and poorly differentiated. The grade is based on how much the tumour cells look like normal squamous cells. A well-differentiated tumour (grade 1) is made up of tumour cells that look almost the same as normal squamous cells. A moderately differentiated tumour (grade 2) is made up of tumour cells that clearly look different from normal squamous cells, however, they can still be recognized as squamous cells. A poorly differentiated tumour (grade 3) is made up of tumour cells that look very little like normal squamous cells. These cells can look so abnormal that your pathologist may need to order an additional test such as immunohistochemistry to confirm the diagnosis. The grade is important because less differentiated tumours (moderately and poorly differentiated tumours) behave in a more aggressive manner and are more likely to spread to other parts of the body.
What does the depth of invasion mean and why is it important for HPV-associated squamous cell carcinoma of the penis?
HPV-associated squamous cell carcinoma starts from squamous cells found in the skin on the surface of the penis. As the tumour grows, the cancer cells can spread into the layers of tissue below the skin. These layers include the lamina propria, dermis, dartos fascia, corpus spongiosum, corpus cavernosum, tunica albuginea, and Buck’s facia. Depth of invasion describes how far the cancer cells have spread from the skin into the layers of tissue below.

The depth of invasion is important because tumours with a greater depth of invasion are more likely to spread to lymph nodes in the pelvis or abdomen. The depth of invasion is also used to determine the pathologic tumour stage (pT).
What is perineural invasion?
Perineural invasion is a term pathologists use to describe cancer cells attached to or inside a nerve. Nerves are like long wires made up of groups of cells called neurons. Nerves are found all over the body and they are responsible for sending information (such as temperature, pressure, and pain) between your body and your brain. Perineural invasion is important because the cancer cells can use the nerve to spread into surrounding organs and tissues. This increases the risk that the tumour will regrow after treatment.

What is lymphovascular invasion?
Lymphovascular invasion means that cancer cells were seen inside of a blood vessel or lymphatic vessel. Blood vessels are long thin tubes that carry blood around the body. Lymphatic vessels are similar to small blood vessels except that they carry a fluid called lymph instead of blood. Lymphovascular invasion is important because cancer cells can use blood vessels or lymphatic vessels to spread to other parts of the body such as lymph nodes or the lungs. For HPV-associated SCC of the penis lymphovascular invasion is also used to determine the pathologic tumour stage (pT).

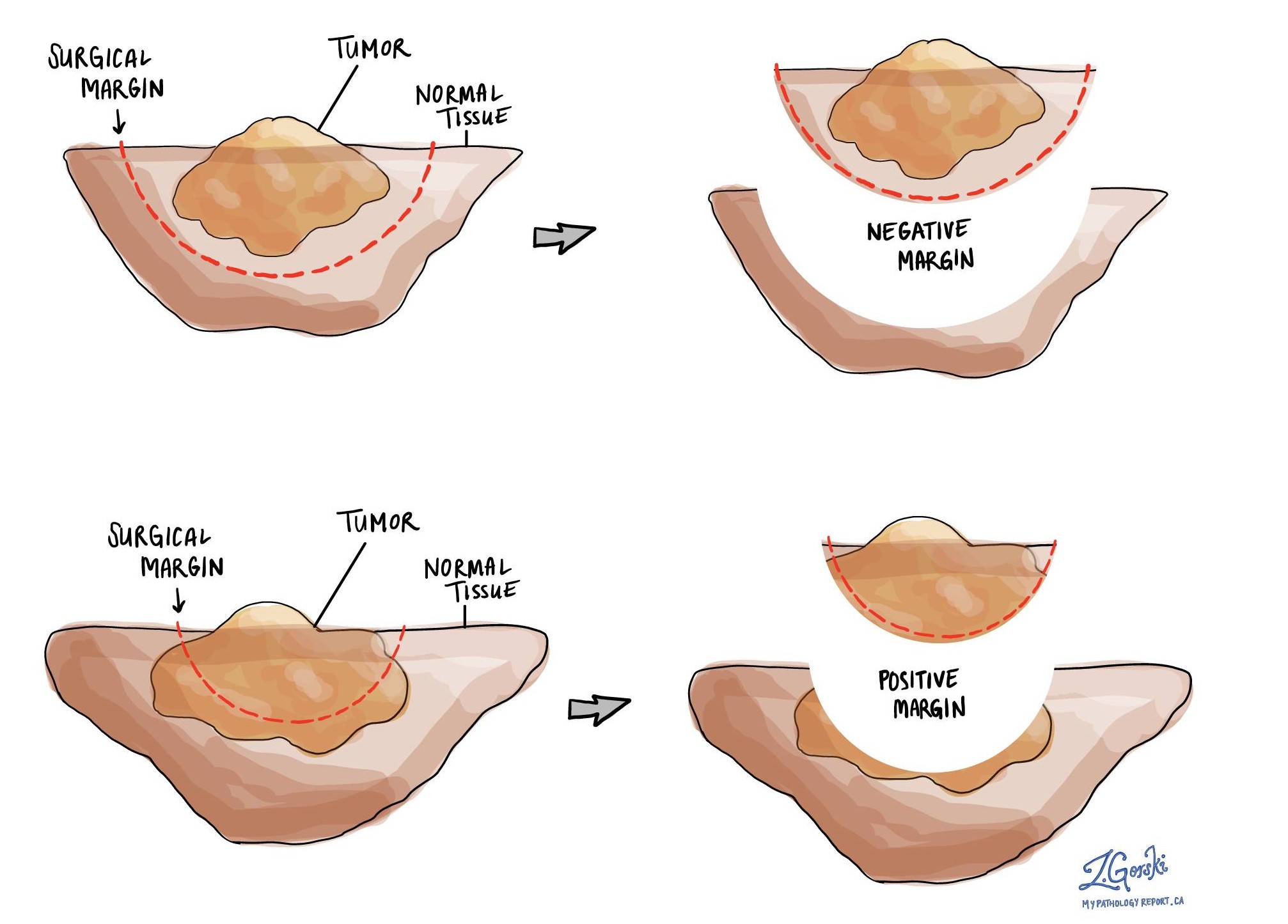
What is a margin?
A margin is any tissue that was cut by the surgeon in order to remove the tumour from your body. The types of margins described in your report will depend on the location of the tumour and the type of surgery performed. Margins will only be described in your report after the entire tumour has been removed.
A negative margin means that no cancer cells were seen at any of the cut edges of tissue. A margin is called positive when there are cancer cells at the very edge of the cut tissue. A positive margin is associated with a higher risk that the tumour will grow back in the same location after treatment.
Were lymph nodes examined and did they contain any cancer cells?
Lymph nodes are small immune organs located throughout the body. Cancer cells can spread from the tumour to a lymph node through lymphatic vessels located in and around the tumour. The movement of cancer cells from the tumour to a lymph node is called metastasis. Lymph nodes from the inguinal canal or pelvis may be removed to look for cancer cells. This information is then used to determine the pathologic nodal stage (pN).
If lymph nodes were removed, your pathologist will examine each lymph node for cancer cells. Lymph nodes that contain cancer cells are called positive while those that do not contain any cancer cells are called negative. Most reports include the total number of lymph nodes examined and the number, if any, that contain cancer cells.
We are proud to partner with:
![]()