

by Jason Wasserman MD PhD FRCPC
May 20, 2026
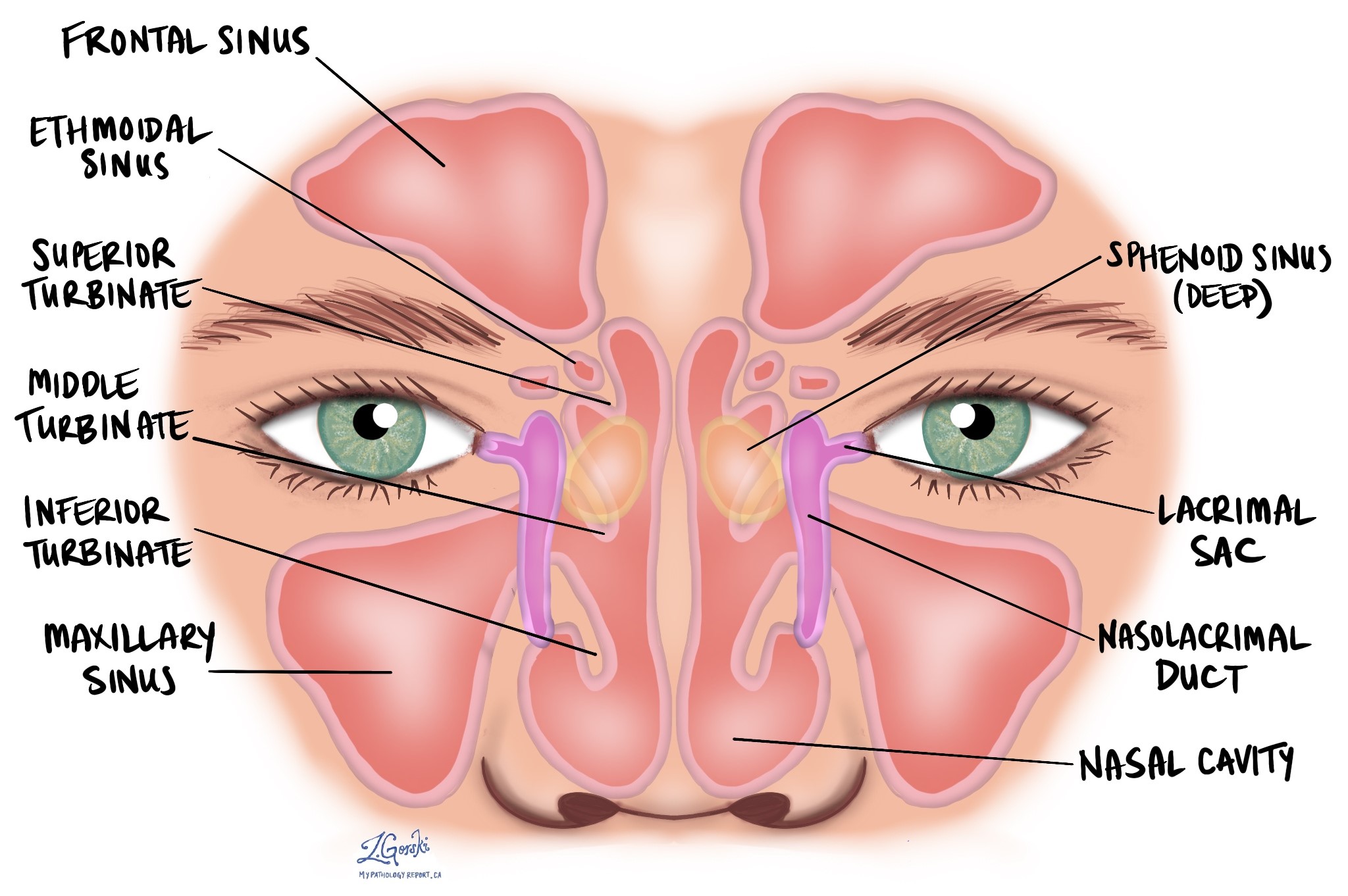
Intestinal-type sinonasal adenocarcinoma (ITAC) is a rare cancer that starts from the tissue lining the inside of the nasal cavity or the paranasal sinuses. The paranasal sinuses are small, air-filled spaces in the bones around the nose, including the ethmoid sinuses (between the eyes) and the maxillary sinuses (beneath the cheeks). ITAC gets its name because, when examined under the microscope, the cancer cells closely resemble those seen in adenocarcinoma of the colon — the part of the large intestine also known as the large bowel.
This article will help you understand the findings in your pathology report, what each term means, and why it matters for your care.
What causes intestinal-type sinonasal adenocarcinoma?
Long-term occupational exposure to certain types of dust is the most well-established risk factor for ITAC. Prolonged exposure to wood dust (especially hardwoods such as oak and beech), leather dust, textile dust, or formaldehyde can damage the cells lining the nasal cavity and sinuses over many years, eventually leading to cancer. Woodworkers, furniture makers, leather workers, and shoe manufacturers are among those at the highest risk. Not all patients with ITAC have this type of work history, and in some cases, no clear cause is identified.
What are the symptoms?
Common symptoms of ITAC include a persistently blocked or stuffy nose, frequent nosebleeds, a decreased sense of smell, and facial pain or pressure. If the tumor has grown close to the eye socket, patients may notice swelling around the eye, double vision, or other changes in vision. Headaches may develop if the tumor has expanded toward the base of the skull. Because the nasal cavity and sinuses are internal structures, early symptoms can be subtle and are often mistaken for chronic sinusitis, which may delay the diagnosis.
How is the diagnosis made?
The diagnosis of ITAC is made after a tissue sample is examined under the microscope by a pathologist. The sample is usually obtained through a biopsy, in which a small piece of tissue is removed from inside the nasal cavity or sinus using an endoscope (a thin, flexible scope passed through the nose). If the tumor is surgically removed in its entirety — a procedure called a resection — the pathologist examines that larger specimen as well.
Under the microscope, ITAC looks very similar to adenocarcinoma of the colon. The tumor cells connect together to form round structures called glands or long finger-like projections called papillae. The glands may be tightly packed in a pattern described by pathologists as cribriform. A type of cell death called necrosis is commonly seen inside the glands. Pathologists sometimes use the term “dirty necrosis” to describe this appearance, which is a characteristic feature of intestinal-type cancers.
Because ITAC looks so similar to a cancer that has spread (metastasized) from somewhere else in the digestive tract, the pathologist will review imaging and your medical history to make sure there is no primary cancer in the colon or elsewhere in the gastrointestinal tract before making this diagnosis. Immunohistochemistry (IHC) is also typically performed. IHC uses specially labeled antibodies to identify specific proteins inside the tumor cells. In ITAC, the tumor cells are usually positive for proteins normally found in the colon, including CK20, CDX-2, and villin. The tumor cells may also be positive for CK7. Together, the imaging review, clinical history, and IHC results allow the pathologist to confirm the diagnosis. Once the diagnosis is established, imaging — typically CT and MRI of the head and neck — is used to assess the full extent of the tumor.
Histologic subtype
Pathologists classify ITAC into five subtypes based on how the tumor cells are arranged under the microscope. The subtype is reported in your pathology report and helps predict how the cancer is likely to behave.
- Papillary type — The tumor grows as finger-like projections (papillae) lined by columnar (column-shaped) cells. This subtype is associated with the most favorable outcomes among all ITAC subtypes.
- Colonic type — The tumor resembles conventional colon adenocarcinoma, with glands lined by columnar cells and dirty necrosis inside the glands. This is the most common subtype and carries an intermediate prognosis.
- Solid type — The tumor cells grow in solid sheets with little or no gland formation. This subtype is associated with the least favorable outcomes.
- Mucinous type — The tumor produces large amounts of mucin, a gel-like substance, which pools around the tumor cells. A variant of this subtype contains signet-ring cells — cells whose nucleus is pushed to one side by mucin filling the interior.
- Mixed type — The tumor shows features of more than one subtype within the same sample.
Perineural invasion
Perineural invasion means that cancer cells were seen attached to or growing along the outside of a nerve. Nerves are found throughout the head and neck and carry signals between the body and the brain. Perineural invasion is an important finding because cancer cells can use nerves as pathways to spread into surrounding tissues, increasing the risk of tumor recurrence after treatment. If perineural invasion is present, it will be described in your pathology report.
Lymphovascular invasion
Lymphovascular invasion means that cancer cells were observed within a blood or lymphatic vessel. Blood vessels carry blood throughout the body, and lymphatic vessels carry a fluid called lymph. Both types of vessels connect different parts of the body, and cancer cells that enter them can travel to distant sites such as lymph nodes or the lungs. If lymphovascular invasion is present, it will be included in your pathology report.
Surgical margins
A surgical margin is the edge of the tissue that the surgeon cuts through when removing a tumor. After surgery, the pathologist examines the margins carefully to look for cancer cells at the cut edges of the tissue. Because ITAC is sometimes removed in multiple separate pieces during surgery, the pathologist may not be able to assess all margins in every case.
- Negative margin — No cancer cells are present at the cut edge of the tissue. This suggests the tumor was completely removed.
- Close margin — Cancer cells are present near the cut edge but do not reach it. Even when margins are technically negative, a very close distance may be noted because it can be relevant to decisions about additional treatment.
- Positive margin — Cancer cells are present at the cut edge of the tissue. This means some tumor may remain in the body, and the treatment team will use this information when considering whether additional surgery or radiation therapy is appropriate.
Lymph nodes
Lymph nodes are small immune organs found throughout the body, including the neck. Cancer cells can spread from a tumor in the nasal cavity or sinuses through lymphatic vessels to nearby lymph nodes. When lymph nodes are removed during surgery, they are examined under the microscope and the results are described in your pathology report.
Your report will include the total number of lymph nodes examined, the number (if any) that contain cancer cells, and the size of the largest group of cancer cells (often called a “focus” or “deposit”). A lymph node that contains cancer cells is described as “positive,” and a lymph node with no cancer cells is described as “negative.”
If cancer cells are found within a lymph node, the pathologist will also assess for extranodal extension. Extranodal extension means that cancer cells have broken through the outer wall (capsule) of the lymph node and spread into the surrounding tissue. In head and neck cancers, extranodal extension is an important finding used to determine the nodal stage and may influence decisions about additional treatment, such as radiation therapy.
Biomarker and molecular testing
Routine biomarker testing is not yet a standard part of every ITAC workup, but one test is increasingly relevant for treatment planning.
Mismatch repair (MMR) and microsatellite instability (MSI)
The mismatch repair (MMR) system is a group of proteins — MLH1, PMS2, MSH2, and MSH6 — that work together inside cells to find and fix small mistakes in DNA. When one or more of these proteins is missing or not working properly, errors accumulate in the cell’s DNA over time. This state is called mismatch repair deficiency (dMMR), also known as microsatellite instability-high (MSI-H).
Because ITAC resembles colon adenocarcinoma under the microscope, some pathologists test ITAC for MMR status. When a tumor is dMMR/MSI-H, it may be eligible for treatment with the immunotherapy drug pembrolizumab (Keytruda) under a tumor-agnostic approval that applies across cancer types, regardless of where the cancer started. A dMMR result also raises the possibility of Lynch syndrome, an inherited condition caused by a change in one of the MMR genes that increases the risk of several cancers. If dMMR is identified in your tumor, your care team may recommend referral for genetic counseling to determine whether Lynch syndrome is the underlying cause.
MMR testing is performed on tumor tissue using immunohistochemistry. This test checks whether each of the four MMR proteins is present or absent in the cancer cells. MSI testing can also be performed using a molecular method that directly examines DNA for errors. Your report will describe which proteins were present or absent, and the overall result will be summarized as MMR-proficient (pMMR) or MMR-deficient (dMMR).
Learn more about MMR and MSI testing at the Biomarkers section of MyPathologyReport, or visit the full Biomarkers and Molecular Testing library.
Pathologic stage (pTNM)
The pathologic stage for ITAC is based on the TNM staging system, as defined in the American Joint Committee on Cancer (AJCC) Cancer Staging Manual, 8th edition. This system describes the tumor using three categories: the primary tumor (pT), regional lymph nodes (pN), and distant spread (pM). In general, a higher stage reflects more advanced disease and is associated with a less favorable outlook. The metastatic stage (pM) is determined by imaging and clinical evaluation, not by the pathologist examining the surgical specimen. Because ITAC can start in different locations — the nasal cavity and ethmoid sinus, or the maxillary sinus — the T stage criteria differ depending on where the tumor began.
Tumor stage (pT) — nasal cavity and ethmoid sinus
- pT1 — The tumor is limited to one area (subsite) within the nasal cavity or ethmoid sinus, with or without involvement of the surrounding bone.
- pT2 — The tumor involves two subsites within the nasal cavity or ethmoid sinus, or has extended into an adjacent area within the nasoethmoidal complex, with or without involvement of the surrounding bone.
- pT3 — The tumor has extended into the inner wall or floor of the orbit (the bony socket that holds the eye), the maxillary sinus, the palate (the roof of the mouth), or the cribriform plate (a bony shelf at the top of the nasal cavity).
- pT4a — The tumor has grown into the front part of the eye socket, the skin of the nose or cheek, a limited area at the base of the skull (anterior cranial fossa), the pterygoid plates (wing-shaped bones at the base of the skull), or the sphenoid or frontal sinuses.
- pT4b — The tumor has grown into the deepest part of the eye socket (orbital apex), the coverings of the brain (dura), the brain itself, the middle cranial fossa, specific cranial nerves, the upper throat behind the nose (nasopharynx), or a bony area at the base of the skull (clivus).
Tumor stage (pT) — maxillary sinus
- pT1 — The tumor is limited to the lining of the maxillary sinus and has not caused any destruction of the surrounding bone.
- pT2 — The tumor has caused erosion or destruction of the bone, including possible spread into the hard palate or a passageway inside the nasal cavity (the middle nasal meatus), but has not reached the back wall of the maxillary sinus or the pterygoid plates.
- pT3 — The tumor has invaded the bone of the back wall of the maxillary sinus, the tissue just beneath the skin (subcutaneous tissue), the floor or inner wall of the orbit, the pterygoid fossa (a depression at the side of the skull base), or the ethmoid sinuses.
- pT4a — The tumor has grown into the front part of the eye socket, the skin of the cheek, the pterygoid plates, the infratemporal fossa (a space at the side of the skull), the cribriform plate, or the sphenoid or frontal sinuses.
- pT4b — The tumor has grown into the deepest part of the eye socket, the coverings of the brain, the brain itself, the middle cranial fossa, specific cranial nerves, the nasopharynx, or the clivus.
Nodal stage (pN) — nasal cavity and paranasal sinuses
- pNX — The lymph nodes could not be assessed.
- pN0 — No cancer cells were found in any of the lymph nodes examined.
- pN1 — Cancer cells were found in a single lymph node on the same side of the neck as the tumor. The lymph node is 3 cm or smaller and shows no extranodal extension.
- pN2a — Cancer cells were found in a single lymph node on the same side of the neck. The lymph node is larger than 3 cm but no larger than 6 cm, and shows no extranodal extension.
- pN2b — Cancer cells were found in more than one lymph node on the same side of the neck. None of the involved lymph nodes is larger than 6 cm, and none shows extranodal extension.
- pN2c — Cancer cells were found in lymph nodes on both sides of the neck, or on the opposite side from the tumor. None of the involved lymph nodes is larger than 6 cm, and none shows extranodal extension.
- pN3a — A lymph node containing cancer cells is larger than 6 cm and shows no extranodal extension.
- pN3b — Cancer cells are present in one or more lymph nodes with obvious extranodal extension.
What is the prognosis?
Prognosis refers to the likely long-term outcome after a diagnosis. For ITAC overall, the five-year survival rate is approximately 40 to 60 percent, though outcomes vary considerably depending on several factors. Histologic subtype is one of the strongest predictors: the papillary subtype is associated with the most favorable outcomes, whereas the solid subtype is associated with the least favorable prognosis. The colonic subtype falls in between.
Stage at diagnosis is also strongly linked to outcomes. Tumors diagnosed at an earlier stage, before they have spread outside the nasal cavity or sinuses, are more likely to be completely removed with surgery. Advanced tumors that involve the base of the skull, the orbit, or the brain are harder to treat surgically and carry a higher risk of recurrence. The presence of lymph node involvement, perineural invasion, lymphovascular invasion, or positive surgical margins also increases the risk of the tumor returning after treatment.
What happens after the diagnosis?
Treatment planning for ITAC typically involves a multidisciplinary team that may include ear, nose, and throat (ENT) surgeons, neurosurgeons (for tumors near the skull base), radiation oncologists, and medical oncologists. The approach is guided by the stage, location, and extent of the tumor, as well as findings from the pathology report.
Surgery is the primary treatment for most patients with ITAC that can be removed. Depending on the extent of disease, surgery may be performed endoscopically (through the nose using a thin scope) or through a larger open surgical approach involving the face and skull base. The goal of surgery is the complete removal of the tumor with clear margins.
Radiation therapy is commonly given after surgery, particularly when surgical margins are close or positive, when perineural invasion is present, or when lymph nodes contain cancer cells. These specific findings from the pathology report directly inform decisions about whether to add radiation therapy and how it is planned.
For locally advanced or metastatic disease, chemotherapy using platinum-based regimens may be considered, often borrowing from protocols used in colorectal cancer. For tumors found to be MMR-deficient (dMMR) or microsatellite instability-high (MSI-H), immunotherapy with pembrolizumab may be an option based on the tumor-agnostic approval that applies across cancer types.
Questions to ask your doctor
- Where exactly did my cancer start — in the nasal cavity, ethmoid sinus, or maxillary sinus?
- What histologic subtype of ITAC was found in my report, and what does that mean for my prognosis?
- What is my pathologic stage (pT and pN), and what does that mean for my treatment?
- Were the surgical margins negative, and does the report suggest all of the tumor was removed?
- Was perineural invasion present in my tumor?
- Was lymphovascular invasion present in my tumor?
- Were lymph nodes examined, and did any contain cancer cells? Was extranodal extension present?
- Was MMR or MSI testing performed on my tumor, and what were the results?
- Will I need radiation therapy after surgery, and what findings in my pathology report influenced that recommendation?
- Based on my MMR results, is there any concern about Lynch syndrome, and should I be referred for genetic counseling?
- What signs of recurrence should I watch for, and how will I be monitored after treatment?
- Are there any clinical trials available for my type of cancer?
Related articles
We are proud to partner with:
![]()