

by Jason Wasserman MD PhD FRCPC and Zuzanna Gorski MD
January 17, 2024
Invasive adenocarcinoma of the rectum (also known as rectal adenocarcinoma) is the most common type of rectal cancer. It is made up of cells that normally cover the inside surface of the rectum. This type of cancer often starts in a polyp such as a tubular adenoma, tubulovillous adenoma, or villous adenoma.
This article will help you understand your diagnosis and pathology report for invasive adenocarcinoma of the rectum.
The rectum
The rectum is part of the digestive system and the final straight segment of the large intestine. It is located just after the sigmoid colon and it connects to the anus. In adults, the rectum is approximately 12 to 15 centimetres long. Its size and shape can vary among individuals.
The primary function of the rectum is to store feces until it can be expelled from the body. When the rectum is full, stretch receptors in its walls trigger the urge to defecate. This process involves the relaxation of the internal and external anal sphincters, along with a series of muscular contractions to expel the contents.

Invasive adenocarcinoma of the rectum
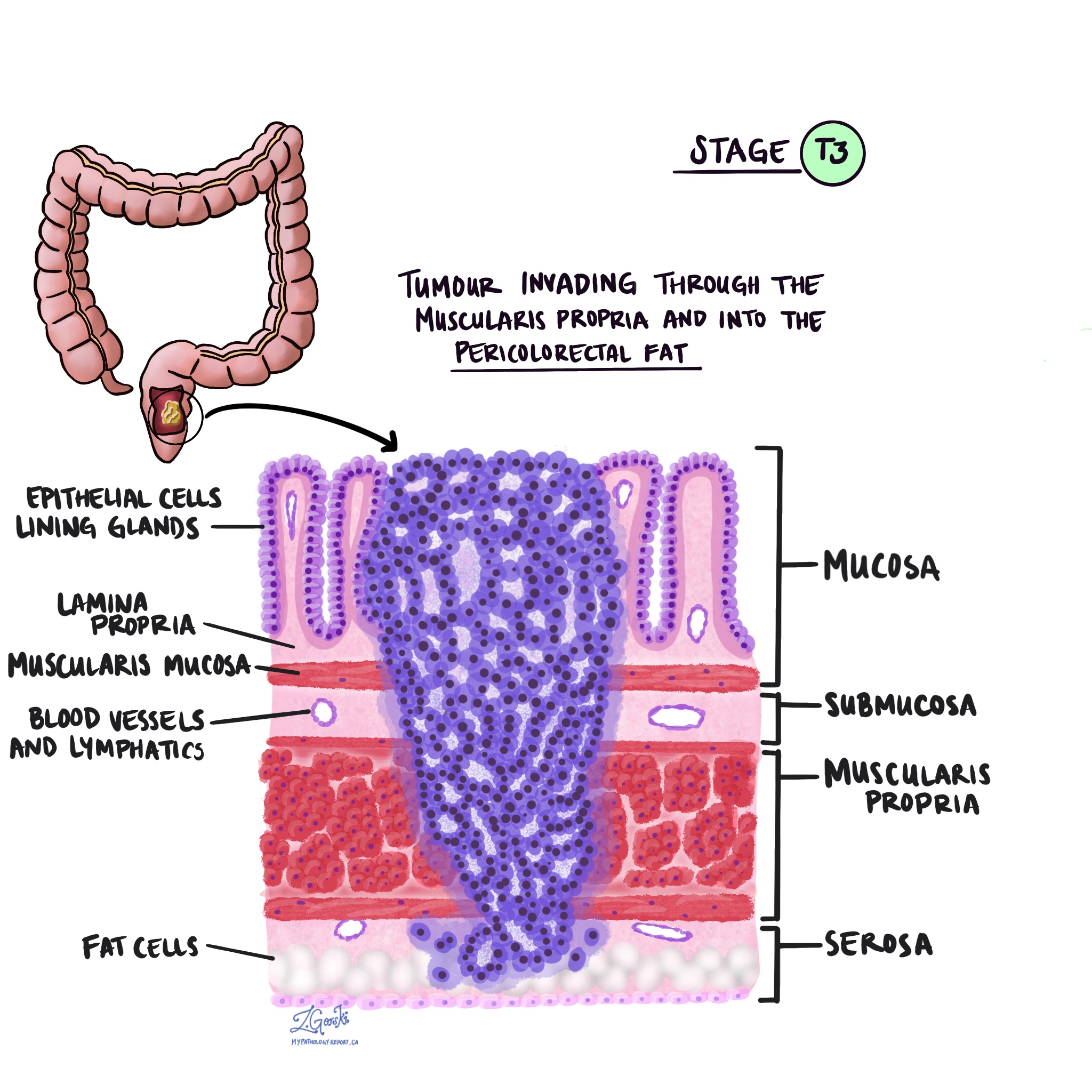
Invasive adenocarcinoma of the rectum is made up of epithelial cells that are normally found on the inside surface of the rectum. These epithelial cells connect to form structures called glands. The glands together with the underlying lamina propria and muscularis mucosae form a thin layer of tissue called the mucosa. When the tumour cells are located entirely within the mucosa, the condition is called high grade dysplasia.
High grade dysplasia is considered a non-invasive, precancerous condition and the tumour cells are unable to metastasize (spread) to other parts of the body. However, as the tumour grows and the cells invade the underlying layers of tissue, the diagnosis changes to invasive adenocarcinoma. In contrast to high grade dysplasia, the tumour cells in invasive carcinoma can metastasize (spread) to lymph nodes and other parts of the body.
What causes invasive adenocarcinoma in the rectum?
Invasive adenocarcinoma in the rectum is believed to be caused by a combination of environmental and genetic factors. Established risk factors include excess consumption of processed meats, red meats, and alcohol. People with excess body fat are also at increased risk of developing this type of cancer. Prolonged inflammation in the rectum, which can be seen in inflammatory bowel disease (ulcerative colitis and Crohn’s disease), is also associated with an increased risk of developing invasive adenocarcinoma.
What are the symptoms of invasive adenocarcinoma of the rectum?
Symptoms of invasive adenocarcinoma of the rectum include changes in bowel habits, bloody stools, abdominal pain, and bloating.
Your pathology report for invasive adenocarcinoma of the rectum
The information found in your pathology report for invasive adenocarcinoma of the rectum will depend on the type of procedure performed. For example, the information found in a report after a biopsy is performed is usually limited to the diagnosis although some reports may also describe the results of additional tests such as mismatch repair proteins (see section below for more information). After the entire tumour has been removed, your pathology report will include additional information such as the tumour grade, depth of invasion, presence or absence of lymphovascular and perineural invasion, and the assessment of margins. The results of any lymph nodes examined should also be included in this final report. If you received treatment such as chemotherapy or radiation therapy before surgery, your pathology report will also describe the response to treatment. These topics are described in more detail in the sections below.
Mucinous differentiation
Pathologists use the term mucinous differentiation to describe tumours that contain a large amount of extracellular mucin. Mucin is a specialized type of protein made by both normal cells and tumour cells. Extracellular means that the mucin was seen outside of the tumour cells. If more than 50% of the tumour is made up of mucin, the tumour is called mucinous adenocarcinoma.
Tumour grade
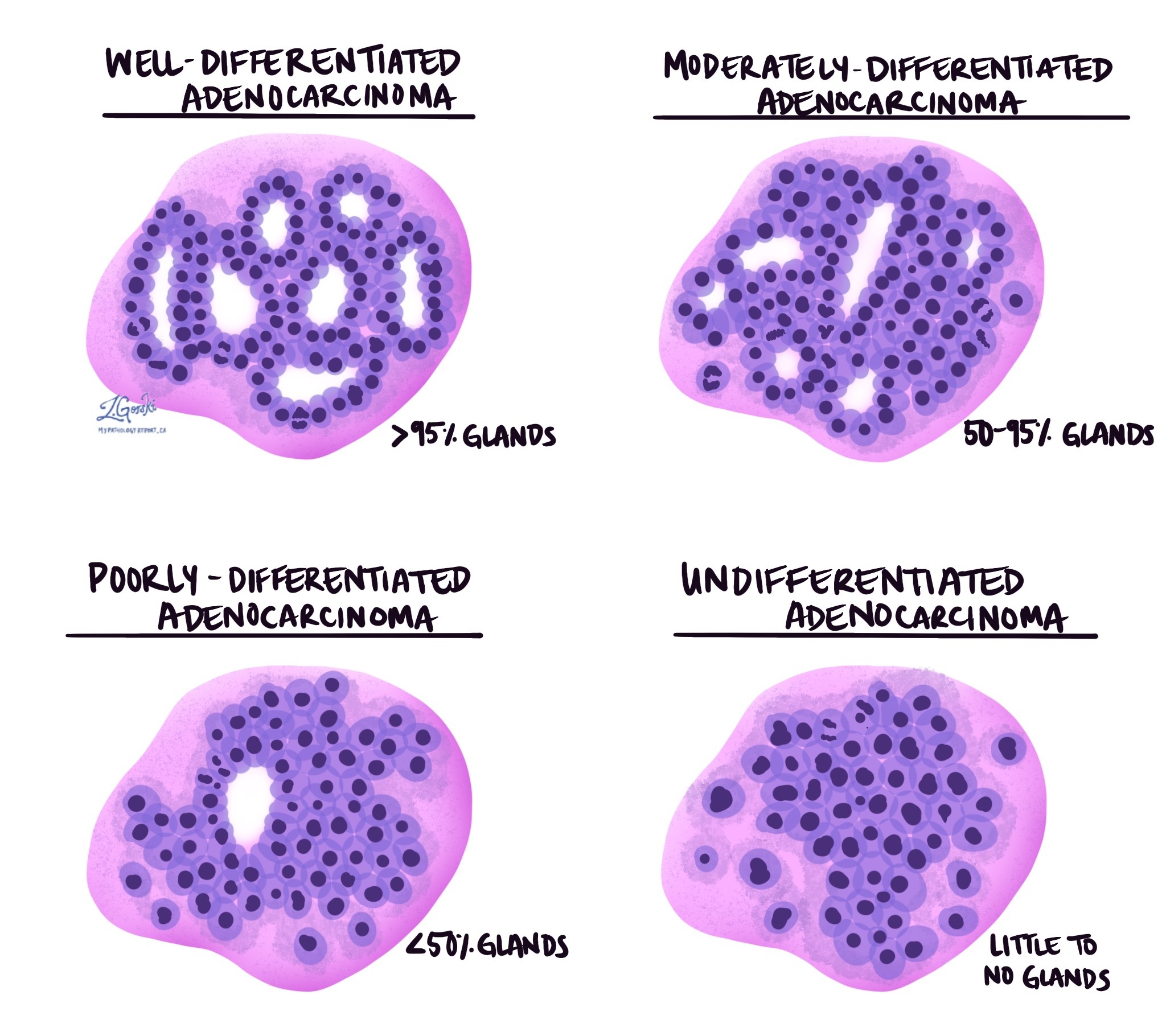
Invasive adenocarcinoma of the rectum is divided into three grades – well differentiated, moderately differentiated, and poorly differentiated. The grade is based on the percentage of the tumour cells forming round structures called glands. A tumour that does not form any glands is called undifferentiated. The grade is important because poorly differentiated and undifferentiated tumours tend to behave more aggressively, for example, these tumours are more likely to spread to lymph nodes and other parts of the body.
- Well differentiated: More than 95% of the tumour is made up of glands. Pathologists also describe these tumours as grade 1.
- Moderately differentiated: 50 to 95% of the tumour is made up of glands. Pathologists also describe these tumours as grade 2.
- Poorly differentiated: Less than 50% of the tumour is made up of glands. Pathologists also describe these tumours as grade 3.
- Undifferentiated: Very few glands are seen anywhere in the tumour.
Depth of invasion
In pathology, the term invasion is used to describe the spread of cancer cells into organs or tissues surrounding the location where the tumour started. Because invasive adenocarcinoma starts in a thin layer of tissue on the inside surface of the rectum called the mucosa, invasion is defined as the spread of cancer cells into the other layers of tissue in the rectum or any other organs outside of the rectum. Invasion can only be seen after the tumour has been examined under a microscope by a pathologist.
When examining the tumour under the microscope, your pathologist will look to see how far the cancer cells have spread from the mucosa into the surrounding tissue. This is called the depth of invasion. The depth of invasion is important because tumours that invade deeper into the wall of the colon are more likely to spread to other parts of the body such as lymph nodes, the liver, or the lungs. The depth of invasion is also used to determine the pathologic tumour stage (pT).



Perineural invasion
Pathologists use the term “perineural invasion” to describe a situation where cancer cells attach to or invade a nerve. “Intraneural invasion” is a related term that specifically refers to cancer cells found inside a nerve. Nerves, resembling long wires, consist of groups of cells known as neurons. These nerves, present throughout the body, transmit information such as temperature, pressure, and pain between the body and the brain. The presence of perineural invasion is important because it allows cancer cells to travel along the nerve into nearby organs and tissues, raising the risk of the tumour recurring after surgery.

Lymphovascular invasion
Lymphovascular invasion occurs when cancer cells invade a blood vessel or lymphatic channel. Blood vessels, thin tubes that carry blood throughout the body, contrast with lymphatic channels, which carry a fluid called lymph instead of blood. These lymphatic channels connect to small immune organs known as lymph nodes, scattered throughout the body. Lymphovascular invasion is important because it enables cancer cells to spread to other body parts, including lymph nodes or the liver, via the blood or lymphatic vessels. The presence of cancer cells inside a large vein beyond the wall of the colon (outside of the thick bundle of muscle) is associated with a high risk that the cancer cells will eventually be found in the liver.

Margins
In pathology, a margin refers to the edge of tissue removed during tumour surgery. The margin status in a pathology report is important as it indicates whether the entire tumour was removed or if some was left behind. This information helps determine the need for further treatment.
Pathologists typically assess margins following a surgical procedure like an excision or resection, aimed at removing the entire tumour. Margins aren’t usually evaluated after a biopsy, which removes only part of the tumour. The number of margins reported and their size—how much normal tissue is between the tumour and the cut edge—vary based on the tissue type and tumour location.
Pathologists examine margins to check if tumour cells are present at the tissue’s cut edge. A positive margin, where tumour cells are found, suggests that some cancer may remain in the body. In contrast, a negative margin, with no tumour cells at the edge, suggests the tumour was fully removed. Some reports also measure the distance between the nearest tumour cells and the margin, even if all margins are negative.

Tumour budding
Tumour budding is a term pathologists use to describe either single cancer cells or small groups of cancer cells seen at the edge of the tumour. Tumour budding is believed to be a sign that the tumour is becoming less differentiated. A score is assigned, either low, intermediate, or high, based on the number of buds seen under the microscope. A high score is associated with an increased risk that cancer cells will spread to another part of the body.
Treatment effect
If you received treatment (either chemotherapy or radiation therapy or both) for your cancer before the tumour is removed, your pathologist will carefully examine the area of the tissue where the tumour was previously identified to see if any cancer cells are still alive (viable). The most commonly used system describes the treatment effect on a scale of 0 to 3 with 0 being no viable cancer cells (all the cancer cells are dead) and 3 being extensive residual cancer with no apparent regression of the tumour (all or most of the cancer cells are alive).
Tumour deposit
A tumour deposit is a group of cancer cells that are separate from the main tumour but not in a lymph node. Tumour deposits are associated with a higher risk that the tumour cells will spread to another part of the body such as the liver or lungs after treatment. Tumour deposits are also used to determine the pathologic tumour stage (pT).
Lymph nodes
Lymph nodes are small immune organs found throughout the body. Cancer cells can spread from a tumour to lymph nodes through small lymphatic vessels. For this reason, lymph nodes are commonly removed and examined under a microscope to look for cancer cells. The movement of cancer cells from the tumour to another part of the body such as a lymph node is called a metastasis.
Cancer cells typically spread first to lymph nodes close to the tumour although lymph nodes far away from the tumour can also be involved. For this reason, the first lymph nodes removed are usually close to the tumour. Lymph nodes further away from the tumour are only typically removed if they are enlarged and there is a high clinical suspicion that there may be cancer cells in the lymph node.
If any lymph nodes were removed from your body, they will be examined under the microscope by a pathologist and the results of this examination will be described in your report. “Positive” means that cancer cells were found in the lymph node. “Negative” means that no cancer cells were found. If cancer cells are found in a lymph node, the size of the largest group of cancer cells (often described as “focus” or “deposit”) may also be included in your report. Extranodal extension means that the tumour cells have broken through the capsule on the outside of the lymph node and have spread into the surrounding tissue.
The examination of lymph nodes is important for two reasons. First, this information is used to determine the pathologic nodal stage (pN). Second, finding cancer cells in a lymph node increases the risk that cancer cells will be found in other parts of the body in the future. As a result, your doctor will use this information when deciding if additional treatment such as chemotherapy, radiation therapy, or immunotherapy is required.

Mismatch repair proteins
Mismatch repair (MMR) is a system inside all normal, healthy cells for fixing mistakes in our genetic material (DNA). The system is made up of different proteins and the four most common are called MSH2, MSH6, MLH1, and PMS2.
The four mismatch repair proteins MSH2, MSH6, MLH1, and PMS2 work in pairs to fix damaged DNA. Specifically, MSH2 works with MSH6 and MLH1 works with PMS2. If one protein is lost, the pair cannot function normally. A loss of one of these proteins increases the risk of developing cancer.
Pathologists order mismatch repair testing to see if any of these proteins are lost in a tumour. If mismatch repair testing has been ordered on your tissue sample, the results will be described in your pathology report.
Why is testing for mismatch repair proteins important?
Mismatch repair (MMR) testing is performed on rectal cancers for two reasons. First, it is performed to identify patients who may have Lynch syndrome, also known as hereditary nonpolyposis colorectal cancer (HNPCC). Lynch syndrome is a genetic disorder that increases the risk of developing various types of cancer, including rectal cancer, endometrial cancer, ovarian cancer, gastric cancer, and others. Second, it is performed to identify patients who may benefit from specific therapies such as chemotherapy and immunotherapy because MMR-deficient tumours tend to respond better to these medications.
How do pathologists test for mismatch repair proteins?
The most common way to test for mismatch repair proteins is to perform a test called immunohistochemistry. This test allows pathologists to see if the tumour cells are producing all four mismatch repair proteins. A normal result will say that the protein is retained or expressed. An abnormal result will say that there is a loss of the protein or that the protein is deficient.
Pathologic stage
Tumour stage (pT)
The pathologic tumour stage (pT) for invasive adenocarcinoma of the rectum is based on the depth of invasion (how far the tumour cells have spread into the wall of the rectum).
- T1 – The tumour cells have spread into the submucosa just below the mucosa on the inner surface of the rectum.
- T2 – The tumour cells have spread into the muscularis propria of the rectum.
- T3 – The tumour cells have spread into fat near the outer surface of the rectum.
- T4 – The tumour cells have spread into a layer of tissue called the serosa on the outer surface of the rectum or the tumour cells have spread into surrounding organs such as the bladder or abdominal wall.
Nodal stage (pN)
The pathologic nodal stage (pN) for invasive adenocarcinoma of the rectum is based on the number of lymph nodes that contain tumour cells or the presence of tumour deposits outside of a lymph node.
- NX – No lymph nodes were examined.
- N0 – No tumour cells were found in any of the lymph nodes examined.
- N1a – Tumour cells were found in 1 lymph node.
- N1b – Tumour cells were found in 2 or 3 lymph nodes.
- N1c – Tumour cells were not found in any lymph nodes but at least one tumour deposit was found.
- N2a – Tumour cells were found in 4 to 6 lymph nodes.
- N2b – Tumour cells were found in 7 or more lymph nodes.
About this article
This article was written by medical doctors in conjunction with patient advisers. It was designed to help patients read and understand their pathology report for invasive adenocarcinoma of the colon. The sections above explain many of the most common features found in pathology reports for this condition. If you have any questions about this article, please contact us.
We are proud to partner with:
![]()