

by Jason Wasserman MD PhD FRCPC and Sarah Strickland MD FRCPC
October 6, 2025
Invasive ductal carcinoma with apocrine features is a type of breast cancer. This type of breast cancer is composed of large, pink cells that resemble the cells typically found in apocrine-type sweat glands in the skin. Invasive ductal carcinoma with apocrine features is a rare type of cancer, representing approximately 1% of all breast cancers.
What are the symptoms of invasive ductal carcinoma with apocrine features?
Like other types of invasive breast cancer, invasive ductal carcinoma with apocrine features may present as a lump in the breast, changes in breast shape or texture, or nipple discharge. However, these symptoms are not specific to apocrine carcinoma and can be seen with other types of breast cancer as well.
What causes invasive ductal carcinoma with apocrine features?
Invasive ductal carcinoma with apocrine features likely develops from a combination of genetic mutations, hormonal influences, and possibly environmental factors. Unlike most breast cancers, it is typically negative for estrogen and progesterone receptors but often positive for androgen receptors, suggesting a potential role for male hormones like testosterone in its growth. While inherited genetic mutations (like BRCA1 or BRCA2) or general breast cancer risk factors (such as smoking or obesity) may contribute, many cases appear to arise randomly without a clear single cause.
How is this diagnosis made?
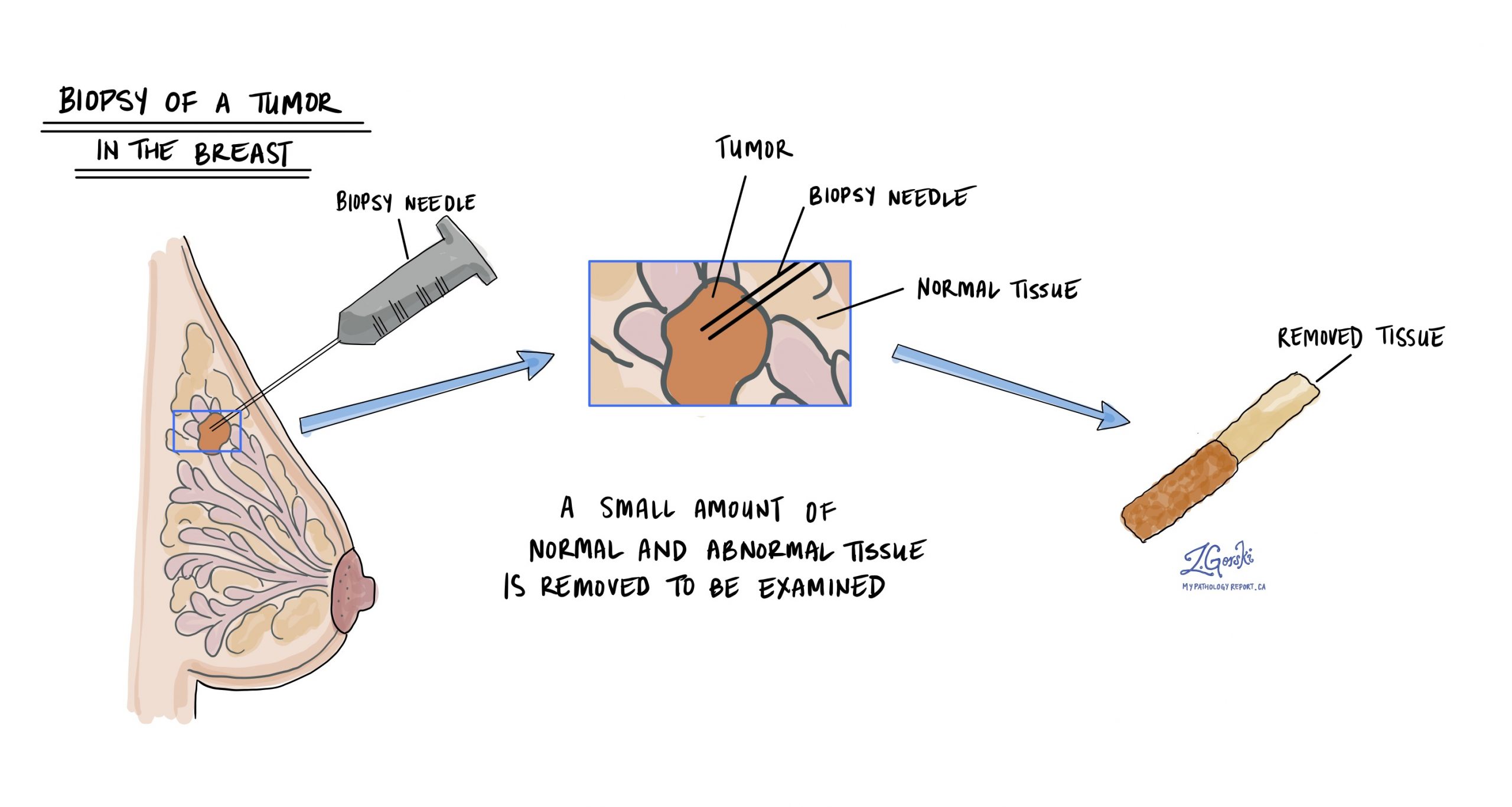
The diagnosis of invasive ductal carcinoma with apocrine features is usually made after a small sample of the tumour is removed in a procedure called a biopsy. The tissue is then sent to a pathologist for examination under a microscope.
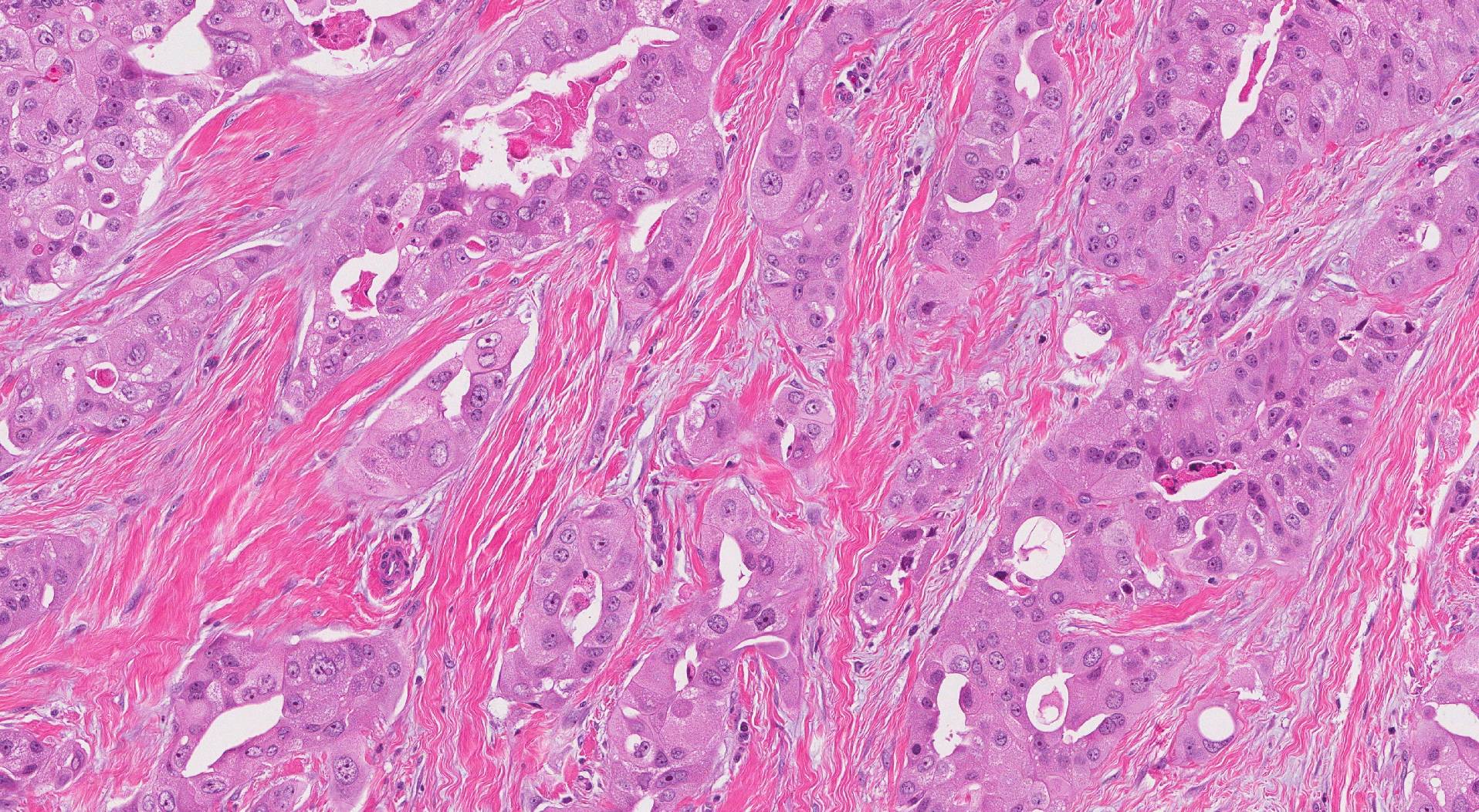
Microscopic features of this tumour
When examined under a microscope, invasive ductal carcinoma with apocrine features comprises large pink cells that look very similar to those found in a type of sweat gland called an apocrine gland. The cells appear pink because the cytoplasm (body of the cell) is full of a protein that sticks to eosin, a pink-coloured dye found in the hematoxylin and eosin (H&E) stain. The cell’s nucleus (the part of the cell that holds the genetic material) tends to be large and round, and clumps of genetic material called nucleoli are often seen. The tumour cells usually produce a protein called androgen receptor (AR), which pathologists can see by performing a test called immunohistochemistry.
Nottingham histologic grade
The Nottingham histologic grade is a system used to assess the aggressiveness of invasive ductal carcinoma with apocrine features by examining the cancer cells under a microscope. The grade is determined by looking at three specific features:
- Tubule formation: This refers to how much of the tumour is made up of round gland-like structures called tubules. Tumors with more tubule formation tend to be less aggressive.
- Nuclear pleomorphism: This describes how abnormal the cancer cell’s nucleus (the part of the cell that contains the DNA) looks compared to normal cells and how much variability there is between cells. The more abnormal it appears, the higher the grade.
- Mitotic rate: This measures how many cells in the tumour are dividing to form new cells. A higher number of mitotic figures suggests a more aggressive tumour.
Each of these features is given a score from 1 to 3, and the scores are added together to determine the final grade:
- Grade 1 (low grade): These tumours grow more slowly and are less likely to metastasize (spread) to lymph nodes.
- Grade 2 (intermediate grade): These tumours grow moderately and are more aggressive, with a higher risk of metastasizing to lymph nodes.
- Grade 3 (high grade): These tumours tend to grow quickly and are associated with a high risk of metastatic disease.
Tumour size
The size of a breast tumour is important because it is used to determine the pathologic tumour stage (pT) and because larger tumours are more likely to metastasize (spread) to lymph nodes and other parts of the body. The tumour size can only be determined after the entire tumour has been removed. For this reason, it will not be included in your pathology report after a biopsy.
Hormone receptors – ER and PR
ER (estrogen receptor) and PR (progesterone receptor) are proteins in some breast cancer cells. These receptors bind to the hormones estrogen and progesterone, respectively. When these hormones attach to their receptors, they can stimulate cancer cells to grow. The presence or absence of these receptors can classify invasive apocrine carcinoma, which is important for determining treatment options and prognosis.
Why is the assessment of ER and PR important?
The presence of ER and PR in breast cancer cells means the cancer is hormone receptor-positive. This type of cancer is often treated with hormone (endocrine) therapy, which blocks the cancer cells’ ability to use hormones. Common hormone therapies include tamoxifen, aromatase inhibitors (such as anastrozole, letrozole, and exemestane), and drugs that lower hormone levels or block the receptors. Hormone receptor-positive cancers often respond well to these therapies.
Hormone receptor-positive breast cancers generally have a better prognosis than hormone receptor-negative cancers. They tend to grow more slowly and are less aggressive. Additionally, hormone receptor-positive cancers are more likely to respond to hormone therapies, which can reduce the risk of recurrence and improve long-term outcomes.
How are ER and PR assessed and reported?
ER and PR status is assessed through immunohistochemistry (IHC), performed on a tumour tissue sample obtained from a biopsy or surgery. The test measures the presence of these hormone receptors inside the cancer cells.
Here’s how the results are typically reported:
- Percentage of positive cells: Your report may include the percentage of cancer cells with ER and PR receptors. For example, a report might state that 80% of the tumour cells are ER-positive and 70% are PR-positive.
- Intensity of staining: Staining intensity (weak, moderate, or strong) reflects the number of receptors present in the nucleus of the cancer cells. This can help determine the likelihood of response to hormone therapy.
- Allred score or H-score: Some reports may use a scoring system like the Allred score or H-score, which combines the percentage of positive cells and the intensity of staining to give an overall score. Higher scores indicate a higher likelihood that hormone therapy will be effective.
HER2
HER2, or human epidermal growth factor receptor 2, is a protein that is found on the surface of some breast cancer cells. It plays a role in cell growth and division. In some breast cancers, the HER2 gene is amplified, leading to an overproduction of the HER2 protein. This condition is referred to as HER2-positive breast cancer.
Why is the assessment of HER2 important?
HER2-positive breast cancers generally have a different prognosis compared to HER2-negative ones. Before the advent of targeted therapies, HER2-positive cancers were associated with a worse prognosis. However, with effective HER2-targeted treatments, the prognosis for these patients has improved significantly. Knowing the HER2 status also helps in planning the overall management of the disease. For instance, in addition to targeted therapy, HER2-positive patients might receive a combination of chemotherapy and other treatments tailored to their specific cancer profile.
How is HER2 assessed in invasive ductal carcinoma with apocrine features?
HER2 status is assessed through tests performed on a tumour tissue sample, which may be obtained through a biopsy or during surgery. The two main tests used are:
- Immunohistochemistry (IHC): This test measures the amount of HER2 protein on the surface of cancer cells. The results are reported as a score from 0 to 3+. A score of 0 or 1+ is considered HER2-negative, 2+ is borderline, and 3+ is HER2-positive.
- Fluorescence in situ hybridization (FISH): This test looks for the number of copies of the HER2 gene within the cancer cells. It is often used to confirm borderline IHC results. If the FISH test shows more copies of the HER2 gene than normal, the cancer is considered HER2-positive.
Tumour extension
Invasive ductal carcinoma with apocrine features starts inside the breast, but the tumour may spread into the overlying skin or the muscles of the chest wall. Tumour extension is used when tumour cells are found in the skin or the muscles below the breast. Tumour extension is important because it is associated with a higher risk that the tumour will grow back after treatment (local recurrence) or that cancer cells will travel to a distant body site such as the lung. Tumour extension is also used to determine the pathologic tumour stage (pT).
Lymphovascular invasion
Lymphovascular invasion (LVI) in the context of invasive ductal carcinoma with apocrine features of the breast refers to cancer cells within the lymphatic vessels or blood vessels near the tumour. This indicates that the cancer can spread beyond its original site through the body’s circulatory systems. LVI can only be identified after a pathologist examines tissue under a microscope. Pathologists look for cancer cells within the lumen of lymphatic or blood vessels, which may appear as clusters or single cells surrounded by a clear space, indicating vessel walls.
The presence of LVI is an important prognostic factor in breast cancer. It is associated with a higher risk of recurrence and metastasis, as the cancer cells can travel to distant parts of the body via the lymphatic system or bloodstream. This finding often prompts a more aggressive treatment approach, which may include additional chemotherapy, radiation therapy, or targeted therapy, depending on other factors such as the overall stage of the cancer, hormone receptor status, and HER2 status.

Margins
In pathology, a margin is the edge of a tissue cut when removing a tumour from the body. The margins described in a pathology report are very important because they tell you if the entire tumour was removed or if some of the tumour was left behind. The margin status will determine what (if any) additional treatment you may require.
Most pathology reports only describe margins after a surgical procedure called an excision or resection has been performed to remove the entire tumour. For this reason, margins are not usually described after a biopsy is performed to remove only part of the tumour. The number of margins described in a pathology report depends on the types of tissues removed and the tumour’s location. The size of the margin (the amount of normal tissue between the tumour and the cut edge) depends on the type of tumour being removed and the location of the tumour.
Pathologists carefully examine the margins to look for tumour cells at the cut edge of the tissue. If tumour cells are seen at the cut edge of the tissue, the margin will be described as positive. If no tumour cells are seen at the cut edge of the tissue, a margin will be described as negative. Even if all of the margins are negative, some pathology reports will also measure the closest tumour cells to the cut edge of the tissue.
A positive (or very close) margin is important because it means that tumour cells may have been left behind in your body when the tumour was surgically removed. For this reason, patients with a positive margin may be offered another surgery to remove the rest of the tumour or radiation therapy to the area of the body with the positive margin.

Lymph nodes
Lymph nodes are small, bean-shaped structures that are part of the immune system. They act as filters, trapping bacteria, viruses, and cancer cells. Lymph nodes contain immune cells that can attack and destroy harmful substances carried in the lymph fluid, which circulates throughout the body.

Why is the examination of lymph nodes important?
Examining lymph nodes is important for understanding the spread of invasive ductal carcinoma with apocrine features. When breast cancer spreads, it often moves first to the nearby lymph nodes before reaching other parts of the body. By examining these lymph nodes, your pathologist can determine whether the cancer has spread beyond the breast. This information is used for cancer staging, planning treatment, and assessing prognosis. If cancer is found in the lymph nodes, it may indicate a higher risk of recurrence and the need for more aggressive treatment.
What lymph nodes are typically examined for patients with invasive ductal carcinoma with apocrine features?
For patients with invasive ductal carcinoma with apocrine features, the lymph nodes that are typically examined include:
- Axillary lymph nodes: These are located under the arm and are the most common lymph nodes examined in breast cancer. They are divided into levels based on their position relative to the pectoral muscles.
- Sentinel lymph nodes: These are the first few lymph nodes to which cancer cells are likely to spread from the primary tumour. A sentinel lymph node biopsy is a procedure in which one or a few nodes are removed and tested for cancer cells.
- Internal mammary lymph nodes: These are located near the breastbone and are sometimes examined, especially if cancer is found in the sentinel lymph nodes or if imaging tests suggest their involvement.
How will the results of the lymph node examination be reported?
The results of the lymph node examination will be detailed in your pathology report.
The report will include information on:
- Number of lymph nodes examined: The total number of lymph nodes removed and examined.
- Number of positive lymph nodes: The number of lymph nodes that contain cancer cells.
- Size of the deposit: Your report will typically include the size of the largest tumour deposit found in a lymph node.
- Other features: Sometimes, additional features, such as extranodal extension (cancer spreading outside the lymph node), will be noted.

What are isolated tumour cells (ITCs)?
Pathologists use the term ‘isolated tumour cells’ to describe a group of tumour cells that measures 0.2 mm or less and is found in a lymph node. Lymph nodes with only isolated tumour cells (ITCs) are not counted as being ‘positive’ for the pathologic nodal stage (pN).
What is a micrometastasis?
A ‘micrometastasis’ is a group of tumour cells measuring 0.2 mm to 2 mm in a lymph node. If only micrometastases are found in all the lymph nodes examined, the pathologic nodal stage is pN1mi.
What is a macrometastasis?
A ‘macrometastasis’ is a group of tumour cells measuring more than 2 mm and found in a lymph node. Macrometastases are associated with a worse prognosis and may require additional treatment.
Treatment effect
If you received treatment (either chemotherapy or radiation therapy) before the tumour was removed, your pathologist will examine all of the tissue submitted to see how much of the tumour is still alive (viable). Lymph nodes with cancer cells will also be examined for treatment effects. A greater treatment effect (no or very few remaining viable tumour cells) is associated with better disease-free and overall survival.
Pathologic stage for invasive ductal carcinoma with apocrine features
The pathologic staging system for invasive ductal carcinoma with apocrine features of the breast helps doctors understand how far the cancer has spread and plan the best treatment. The system mainly uses the TNM staging, which stands for Tumor, Nodes, and Metastasis. Early-stage cancers (like T1 or N0) might only require surgery and possibly radiation, while more advanced stages (like T3 or N3) may need a combination of surgery, radiation, chemotherapy, and targeted therapies. Proper staging ensures that patients receive the most effective treatments based on the extent of their disease, which can improve survival rates and quality of life.
Tumour stage (pT)
This feature examines the size and extent of the breast tumour. The tumour is measured in centimetres, and its growth beyond the breast tissue is assessed.
T0: No evidence of primary tumour. This means no tumour can be found in the breast.
T1: The tumour is 2 centimetres or smaller in greatest dimension. This stage is further subdivided into:
- T1mi: Tumour is 1 millimetre or smaller.
- T1a: Tumor is larger than 1 millimetre but not larger than 5 millimetres.
- T1b: Tumour is larger than 5 millimetres but not larger than 10 millimetres.
- T1c: Tumor is larger than 10 millimetres but not over 20 millimetres.
T2: The tumour is larger than 2 centimetres but not larger than 5 centimetres.
T3: The tumour is larger than 5 centimetres.
T4: The tumour has spread to the chest wall or skin, regardless of its size. This stage is further subdivided into:
- T4a: Tumour has invaded the chest wall.
- T4b: Tumour has spread to the skin, causing ulcers or swelling.
- T4c: Both T4a and T4b are present.
- T4d: Inflammatory breast cancer, characterized by redness and swelling of the breast skin.
Nodal stage (pN)
This feature examines if the cancer has spread to the nearby lymph nodes, which are small, bean-shaped structures found throughout the body.
N0: No cancer is found in the nearby lymph nodes.
N1: Cancer has spread to 1 to 3 axillary lymph nodes (under the arm).
N2: Cancer has spread to:
- N2a: 4 to 9 axillary lymph nodes.
- N2b: Internal mammary lymph nodes without involvement of axillary lymph nodes.
N3: Cancer has spread to:
- N3a: 10 or more axillary lymph nodes or two infraclavicular lymph nodes (below the collarbone).
- N3b: Internal mammary lymph nodes and axillary lymph nodes.
- N3c: Supraclavicular lymph nodes (above the collarbone).
Other helpful resources
American Breast Cancer Foundation
Canadian Breast Cancer Foundation
We are proud to partner with:
![]()