

by Bibianna Purgina MD FRCPC and Jason Wasserman MD PhD FRCPC
January 2, 2024
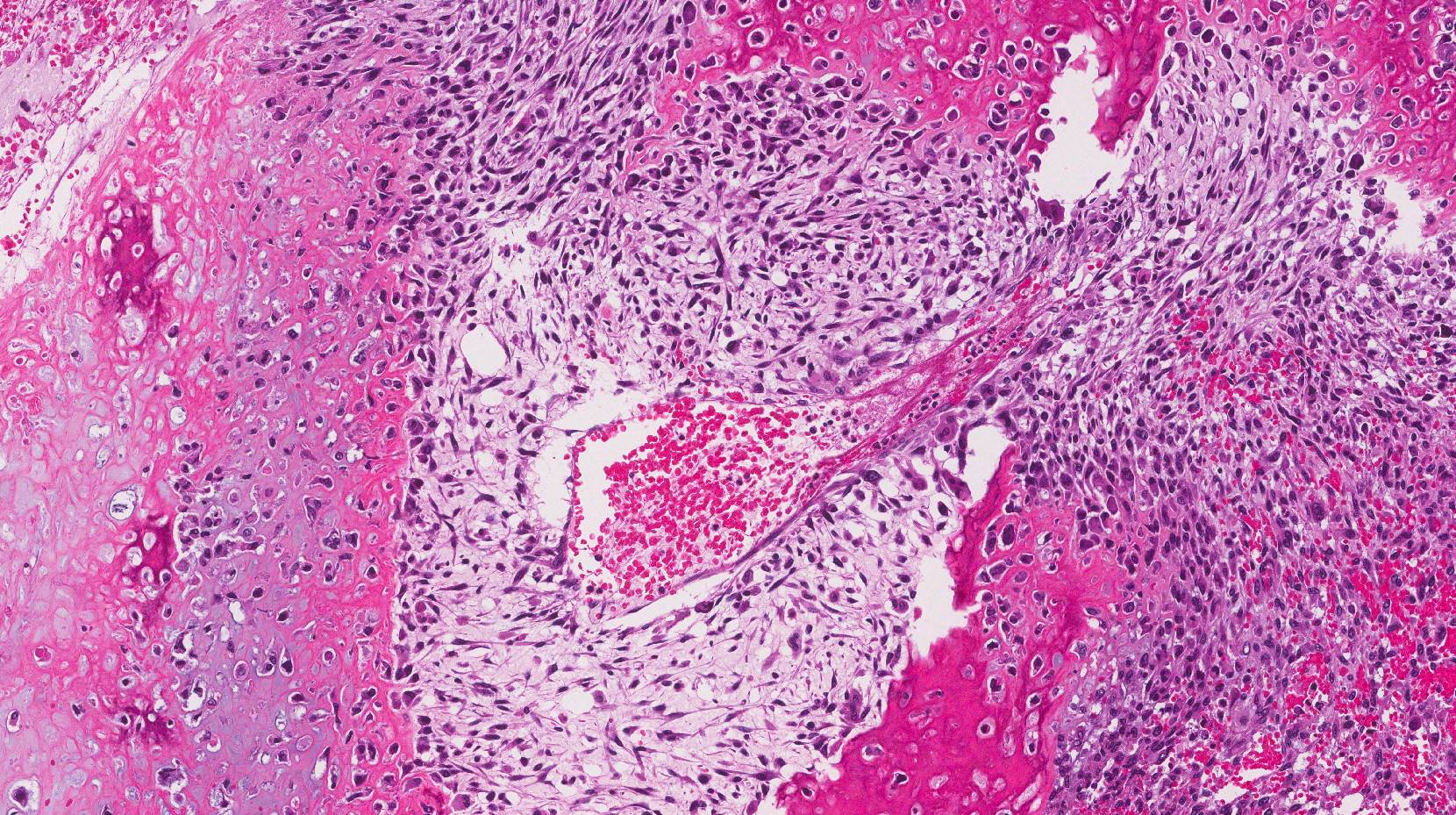
Chondroblastic osteosarcoma is a type of bone cancer. This type of cancer can start in any bone in the body, however, most are found in the long bones of the arms and legs. The jaws are also commonly involved. This type of cancer affects both children and older adults. The term “chondroblastic” means that some areas of the tumour have changed to look like a type of connective tissue called cartilage. The cartilage found in chondroblastic osteosarcoma is called “neoplastic” or “malignant” because it is made by the tumour cells.
What causes chondroblastic osteosarcoma?
For most patients who develop chondroblastic osteosarcoma, the cause remains unknown. However, some genetic syndromes such as Li-Fraumeni syndrome, hereditary retinoblastoma, and Bloom syndrome, increase the risk of developing chondroblastic osteosarcoma.
What are the symptoms of chondroblastic osteosarcoma?
Symptoms of chondroblastic osteosarcoma include a rapidly enlarging and painful mass. As the tumour grows it can cause the bone to fracture (break).
How is this diagnosis made?
The diagnosis of chondroblastic osteosarcoma is typically made after a small tissue sample has been removed in a procedure called a biopsy. After the diagnosis, most patients are treated first with chemotherapy and then with surgery. During surgery, the tumour is removed completely as a resection. The resection specimen is sent to a pathologist for examination. Your pathologist will examine the tumour under the microscope and give your surgeon and oncologist important information that will help guide your treatment.
Tumour grade
All chondroblastic osteosarcomas are considered grade 3 or high-grade tumours. High-grade tumours are aggressive cancers that grow quickly and metastasize (spread) to other parts of the body.
Has the tumour spread outside of the bone?
Pathologists use the term extraosseous extension to describe a bone tumour that has broken through the outside surface of the bone and has spread into the surrounding tissue such as muscles, tendons, or the space around a joint. Extraosseous extension is important because it is associated with a worse prognosis.
What does it mean if the tumour has spread into another bone?
Some bones are made up of multiple parts. If the tumour has grown from one part of a bone into another, your report will describe the tumour as invading adjacent bones. This is particularly important for tumours in the spine or pelvis because both of these bones are made up of multiple parts. Invasion of adjacent bones is important because it is associated with a worse prognosis. It also increases the pathologic tumour stage.
Has the tumour responded to treatment?
If you received chemotherapy before surgery, your pathologist will examine all the tissue sent to pathology to see how much of the tumour is still viable (alive). This is called the treatment effect. Pathologists often measure the treatment effect as the percentage of the tumour that appears dead when examined under the microscope. For example, if the tumour shows a 65% response to therapy, it means that 65% of the tumour is dead. Typically, chondroblastic osteosarcoma showing 90% or more response to therapy (meaning 90% of the tumour is dead and 10% or less of the tumour is still alive) is associated with a better prognosis.
Perineural invasion
Pathologists use the term “perineural invasion” to describe a situation where cancer cells attach to or invade a nerve. “Intraneural invasion” is a related term that specifically refers to cancer cells found inside a nerve. Nerves, resembling long wires, consist of groups of cells known as neurons. These nerves, present throughout the body, transmit information such as temperature, pressure, and pain between the body and the brain. The presence of perineural invasion is important because it allows cancer cells to travel along the nerve into nearby organs and tissues, raising the risk of the tumour recurring after surgery. While it is rare for perineural invasion to be found in chondroblastic osteosarcoma, pathologists always look for it and report it if it is found.

Lymphovascular invasion (angiolymphatic invasion)
Lymphovascular invasion (also known as angiolymphatic invasion) occurs when cancer cells invade a blood vessel or lymphatic channel. Blood vessels, thin tubes that carry blood throughout the body, contrast with lymphatic channels, which carry a fluid called lymph instead of blood. These lymphatic channels connect to small immune organs known as lymph nodes, scattered throughout the body. Lymphovascular invasion is important because it enables cancer cells to spread to other body parts, including lymph nodes or the lungs, via the blood or lymphatic vessels. While it is rare for lymphovascular invasion to be found in chondroblastic osteosarcoma, pathologists always look for it and report it if it is found.

Margins
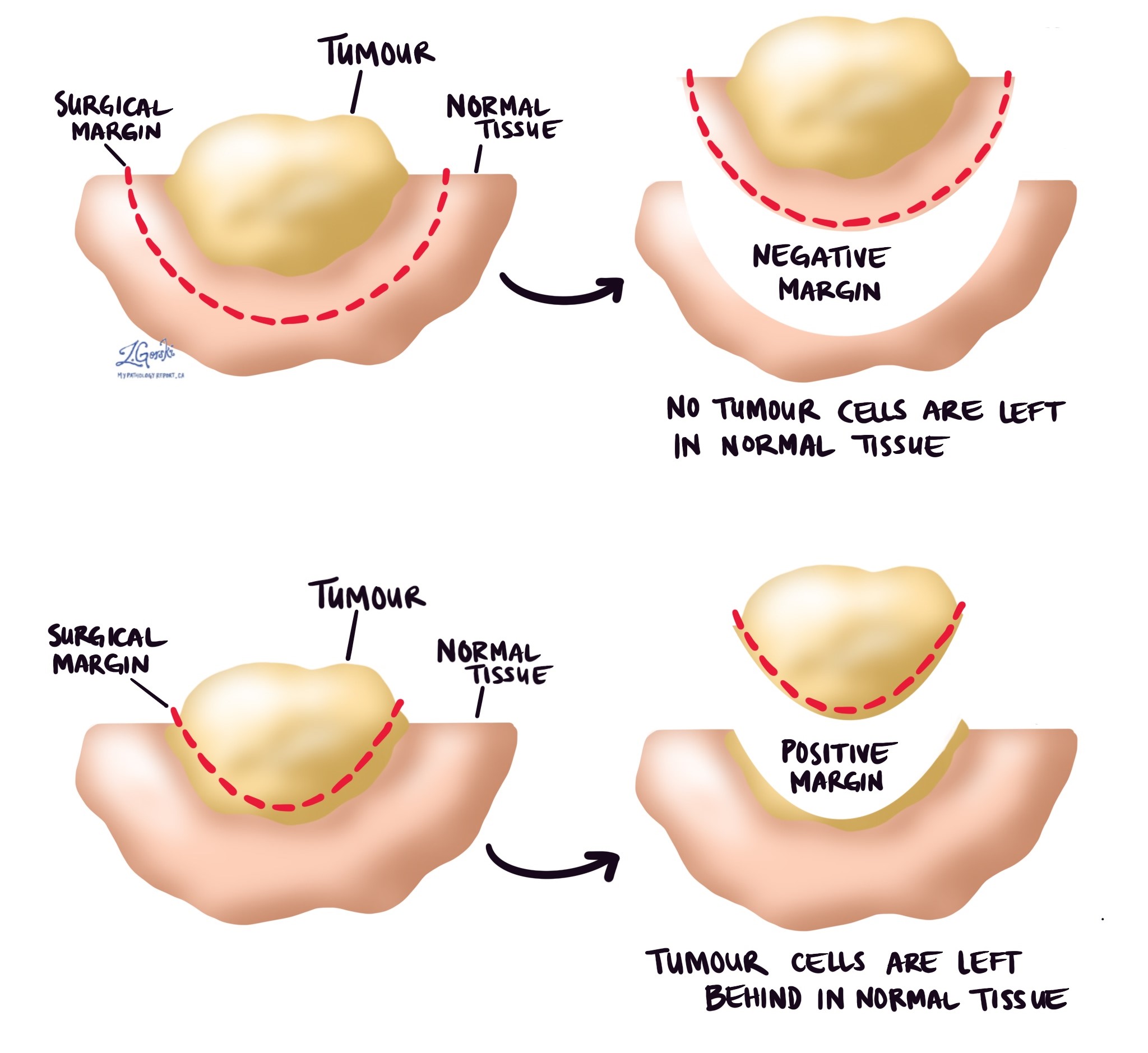
In pathology, a margin refers to the edge of tissue removed during tumour surgery. The margin status in a pathology report is important as it indicates whether the entire tumour was removed or if some was left behind. This information helps determine the need for further treatment.
Pathologists typically assess margins following a surgical procedure like an excision or resection, aimed at removing the entire tumour. Margins aren’t usually evaluated after a biopsy, which removes only part of the tumour. The number of margins reported and their size—how much normal tissue is between the tumour and the cut edge—vary based on the tissue type and tumour location.
Pathologists examine margins to check if tumour cells are present at the tissue’s cut edge. A positive margin, where tumour cells are found, suggests that some cancer may remain in the body. In contrast, a negative margin, with no tumour cells at the edge, suggests the tumour was fully removed. Some reports also measure the distance between the nearest tumour cells and the margin, even if all margins are negative.
Common margins for chondroblastic osteosarcoma include:
- Proximal bone margin – This is the part of the bone closest to the middle of your body.
- Distal bone margin – This is the part of the bone farthest from the middle of your body.
- Soft tissue margins – This is the cut edge of any non-bone tissue that was removed at the same time as the tumour in the bone.
- Blood vessel margins – This is the cut edge of any large blood vessels removed at the same time as the tumour.
- Nerve margins – This is the cut edge of any large nerve removed at the same time as the tumour.
Lymph nodes
Lymph nodes are small immune organs found throughout the body. Cancer cells can spread from a tumour to lymph nodes through small lymphatic vessels. For this reason, lymph nodes are commonly removed and examined under a microscope to look for cancer cells. The movement of cancer cells from the tumour to another part of the body such as a lymph node is called a metastasis.
Cancer cells typically spread first to lymph nodes close to the tumour although lymph nodes far away from the tumour can also be involved. For this reason, the first lymph nodes removed are usually close to the tumour. Lymph nodes further away from the tumour are only typically removed if they are enlarged and there is a high clinical suspicion that there may be cancer cells in the lymph node.
If any lymph nodes were removed from your body, they will be examined under the microscope by a pathologist and the results of this examination will be described in your report. “Positive” means that cancer cells were found in the lymph node. “Negative” means that no cancer cells were found. If cancer cells are found in a lymph node, the size of the largest group of cancer cells (often described as “focus” or “deposit”) may also be included in your report. Extranodal extension means that the tumour cells have broken through the capsule on the outside of the lymph node and have spread into the surrounding tissue.
The examination of lymph nodes is important for two reasons. First, this information is used to determine the pathologic nodal stage (pN). Second, finding cancer cells in a lymph node increases the risk that cancer cells will be found in other parts of the body in the future. As a result, your doctor will use this information when deciding if additional treatment such as chemotherapy, radiation therapy, or immunotherapy is required.

Pathologic stage
The pathologic stage for chondroblastic osteosarcoma is based on a system called the TNM staging system. This system is used around the world and was created by the American Joint Committee on Cancer. This system uses information about the primary tumour (T), lymph nodes (N), and distant metastatic disease (M) to determine the complete pathologic stage (pTNM). Your pathologist will give each category a number after examining your tissue sample under the microscope. In general, a higher number means a more advanced disease and a worse prognosis.
Tumour stage (pT)
For bone cancers such as chondroblastic osteosarcoma, the primary tumour (pT) stage depends on where the tumour is located in your body.
Tumours in the appendicular skeleton
If the tumour is located in your appendicular skeleton (the bones of your arms, legs, shoulder, trunk, skull, or face), it is given a tumour stage of 1, 2 or 3 based on the size of the tumour and whether the tumour was seen in multiple parts of the bone.
- pT1: Tumour is less than or equal to 8 cm.
- pT2: Tumour is greater than 8 cm.
- pT3: Tumour was seen in multiple parts of the bone (discontinuous tumour nodules).
Tumours in the spine
If the tumour is located in your spine, it is given a tumour stage of 1, 2, 3, or 4 based on how far the tumour has grown.
- pT1: Tumour is only seen in one or two adjacent vertebral bones (bones of the spine and the space between them).
- pT2: Tumour is seen in three adjacent vertebral bones.
- pT3: Tumour is seen in four or more adjacent vertebral bones or any nonadjacent vertebral bones.
- pT4: Tumour invades the spinal canal or great vessels.
Tumours in the pelvis
If the tumour is located in your pelvis, it is given a tumour stage of 1, 2, 3, or 4 based on the size of the tumour and how far it has grown.
- pT1: Tumour is in one pelvic bone with no extraosseous extension (tumour is not growing outside of the bone).
- pT1a: Tumour is less than or equal to 8 cm.
- pT1b: Tumour is greater than 8 cm.
- pT2: Tumour is in one pelvic bone with extraosseous extension (tumour is growing outside the bone) or in two bones with no extraosseous extension (tumour is not growing outside the bone).
- pT2a: Tumour is less than or equal to 8 cm.
- pT2b: Tumour is greater than 8 cm.
- pT3: Tumour is in two pelvic bones with extraosseous extension (tumour is growing outside the bone).
- pT3a: Tumour is less than or equal to 8 cm.
- pT3b: Tumour is greater than 8 cm.
- pT4: Tumour is in three pelvic bones or crossing the sacroiliac joint.
- pT4a: Tumour involves the sacroiliac joint and extends into the sacral neuroforamen (space where the nerves pass through).
- pT4b: Tumour surrounds the external iliac vessels or extends into a major pelvic vessel.
Other tumour stages
- pT0: No tumour cells were seen after all of the tissue was examined under the microscope. This means that there is no evidence of a primary tumour.
- pTX (primary tumour cannot be assessed): The pathologist could not determine the tumour size or the distance that it had grown. This may happen if the pathologist receives the tumour as several small pieces.
Nodal stage (pN)
Primary bone cancers are given a nodal stage of 0 or 1 based on whether there are cancer cells in one or more lymph nodes.
- pNX: The pathologist is sent no lymph nodes to examine.
- pN0: No tumour cells are seen in any lymph nodes.
- pN1: Tumour cells are found in one or more lymph nodes.
About this article
This article was written by doctors to help you read and understand your pathology report for chondroblastic osteosarcoma. The sections above describe the results found in most pathology reports, however, all reports are different and results may vary. Importantly, some of this information will only be described in your report after the entire tumour has been surgically removed and examined by a pathologist. Contact us if you have any questions about this article or your pathology report. Read this article for a more general introduction to the parts of a typical pathology report.
Other helpful resources
Atlas of Pathology
We are proud to partner with:
![]()