

by Jason Wasserman MD PhD FRCPC and Zuzanna Gorski MD
April 1, 2025
High grade dysplasia of the larynx, also known as severe keratinizing squamous dysplasia, is a precancerous condition involving the abnormal growth of squamous cells lining the larynx (voice box). Dysplasia means the cells look abnormal when viewed under a microscope and are not developing normally. If left untreated, high grade dysplasia can progress to a type of cancer known as squamous cell carcinoma. This condition usually affects adults over the age of 40.
Is high grade dysplasia invasive?
High grade dysplasia in the larynx is considered a non-invasive condition because the abnormal cells remain within the surface layer of tissue, known as the epithelium. In contrast, squamous cell carcinoma is invasive, meaning the cancer cells have penetrated deeper into the underlying tissues (stroma).

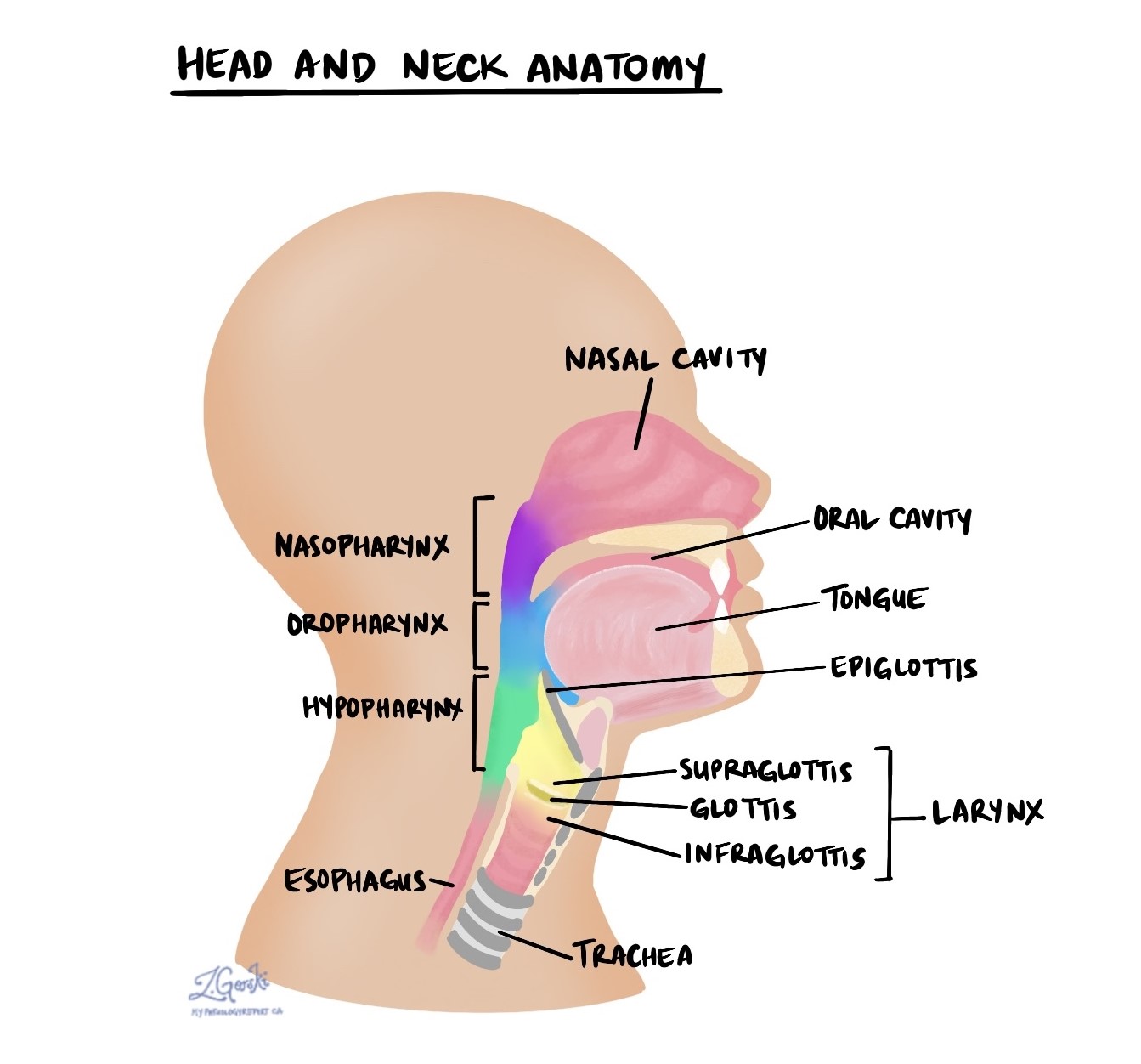
Parts of the larynx
The larynx is located in the upper part of the neck, just above the trachea (windpipe). Its main functions are to protect the airway and produce sound.
The larynx is divided into three parts:
- Supraglottis: the upper part above the vocal cords.
- Glottis: the middle part, including the vocal cords.
- Subglottis: the lower part below the vocal cords.
High grade dysplasia most commonly occurs in the glottis area, especially on the vocal cords. If left untreated, abnormal cells can spread within the larynx, known as transglottic extension.
What causes high grade dysplasia of the larynx?
The leading cause of high grade dysplasia in the larynx is smoking. Other contributing factors include heavy alcohol consumption, immune suppression (weakened immune system), and prior radiation treatment to the neck.
What are the symptoms of high grade dysplasia of the larynx?
Common symptoms of high grade dysplasia of the larynx include:
- Hoarseness or changes in voice quality.
- Difficulty breathing.
- Problems with swallowing.
If you experience any of these symptoms persistently, it’s important to consult a healthcare provider for evaluation.
What is the risk of developing cancer with high grade dysplasia of the larynx?
High grade dysplasia carries a significant risk of developing into squamous cell carcinoma if not treated. Regular monitoring and treatment, such as surgical removal of the abnormal tissue, significantly reduce this risk. The exact risk varies among individuals, and your healthcare provider can give personalized advice based on your situation.
Microscopic features of high grade dysplasia
When viewed under a microscope, high grade dysplasia shows abnormal squamous cells replacing normal, healthy squamous cells in the epithelium (the thin surface layer of tissue). These abnormal cells typically appear larger and hyperchromatic (darker) than normal cells and do not mature normally. A feature known as keratinization may also be present, where abnormal cells produce excessive amounts of keratin, appearing as bright pink or red areas.
Margins
In pathology, margins refer to the edges of tissue removed during surgery. The status of margins is important because it helps determine if all abnormal tissue has been removed or if some remains.
Pathologists carefully examine the margins after surgery to remove abnormal tissue (excision or resection). Margins are usually not assessed after a biopsy, as only a portion of the abnormal tissue is removed.
A margin is considered positive if abnormal cells are present at the cut edge, indicating that some dysplasia or cancer might still be in the body. A negative margin means no abnormal cells were found at the edges, suggesting the condition has been entirely removed. Pathologists may also measure the distance between the abnormal cells and the nearest margin, even if margins are negative, to provide additional information for your treatment planning.

We are proud to partner with:
![]()