

by Bibianna Purgina MD FRCPC
June 7, 2023
What is nodular fasciitis?
Nodular fasciitis is a non-cancerous type of tumour that develops from fibrous tissue. This type of tumour typically occurs in young adults and although they can arise anywhere in the body, it is more common in the head, arm, or back.
Sometimes nodular fasciitis grows quickly which can cause concern for both the patient and their doctor. Even though nodular fasciitis can grow quickly, the tumour is usually less than 3 centimetres in size when it is removed.
As the name suggests, nodular fasciitis is often associated with a thin tissue called fascia. Fascia can be found throughout the body where it surrounds muscles and internal organs. Like most non-cancerous tumours, nodular fasciitis is typically cured by surgical removal.
How do pathologists make this diagnosis?
The initial diagnosis of nodular fasciitis is usually made after a small sample of the tumour is removed in a procedure called a biopsy or if the tumour is removed completely in a procedure called an excision. The tissue is then sent to a pathologist who examines it under a microscope. Additional tests such as immunohistochemistry or molecular testing may also be performed to confirm the diagnosis.
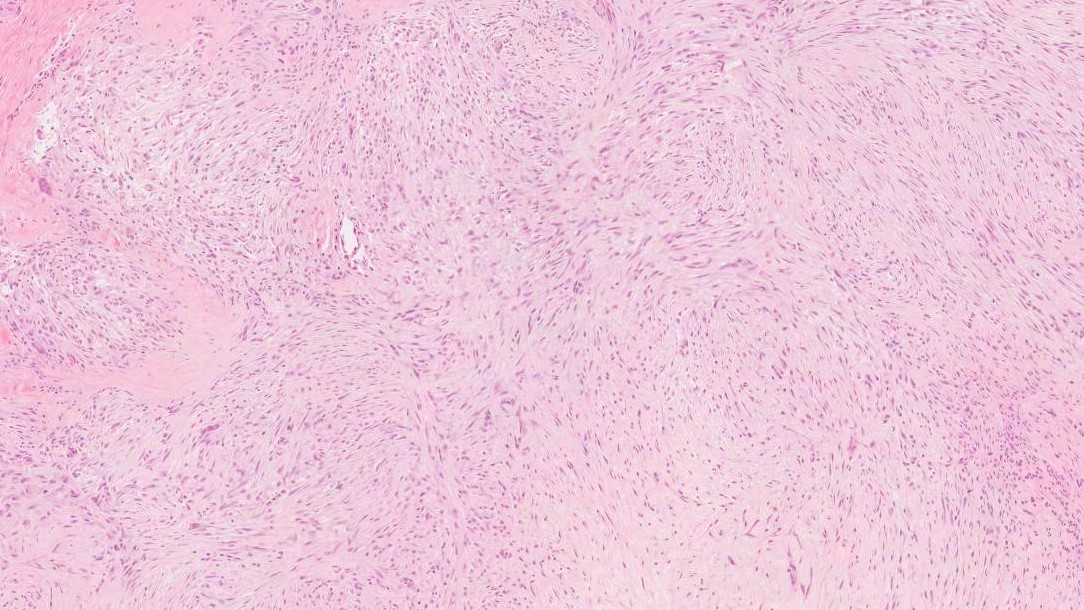
Under the microscope, nodular fasciitis is a well-defined tumour that can have both areas with lots of tumour cells (hypercellular areas) and areas with fewer tumour cells (hypocellular areas). The less cellular areas often bluish-grey look under the microscope which pathologists call myxoid.
The tumour cells of nodular fasciitis look like the cells that make up normal fibrous tissue. These cells are called fibroblasts and myofibroblasts. The fibroblasts and myofibroblasts in nodular fasciitis often look plump and feathery. The appearance of nodular fasciitis is often described as having a “tissue culture”-like growth pattern.
Sometimes a small tissue sample taken from the tumour only shows more cellular areas and the larger tumour cells. In these situations, your pathologist may consider other diagnoses which can include both benign (non-cancerous) tumours and malignant (cancerous) tumours. When this happens, the final diagnosis will not be made until the entire tumour has been removed.
Tumour size
After the tumour is completely removed your pathologist will measure it in three dimensions but only the largest dimension is typically included in your report. For example, if the tumour measures 5.0 cm by 3.2 cm by 1.1 cm, the report may describe the tumour size as 5.0 cm in the greatest dimension.
Margins
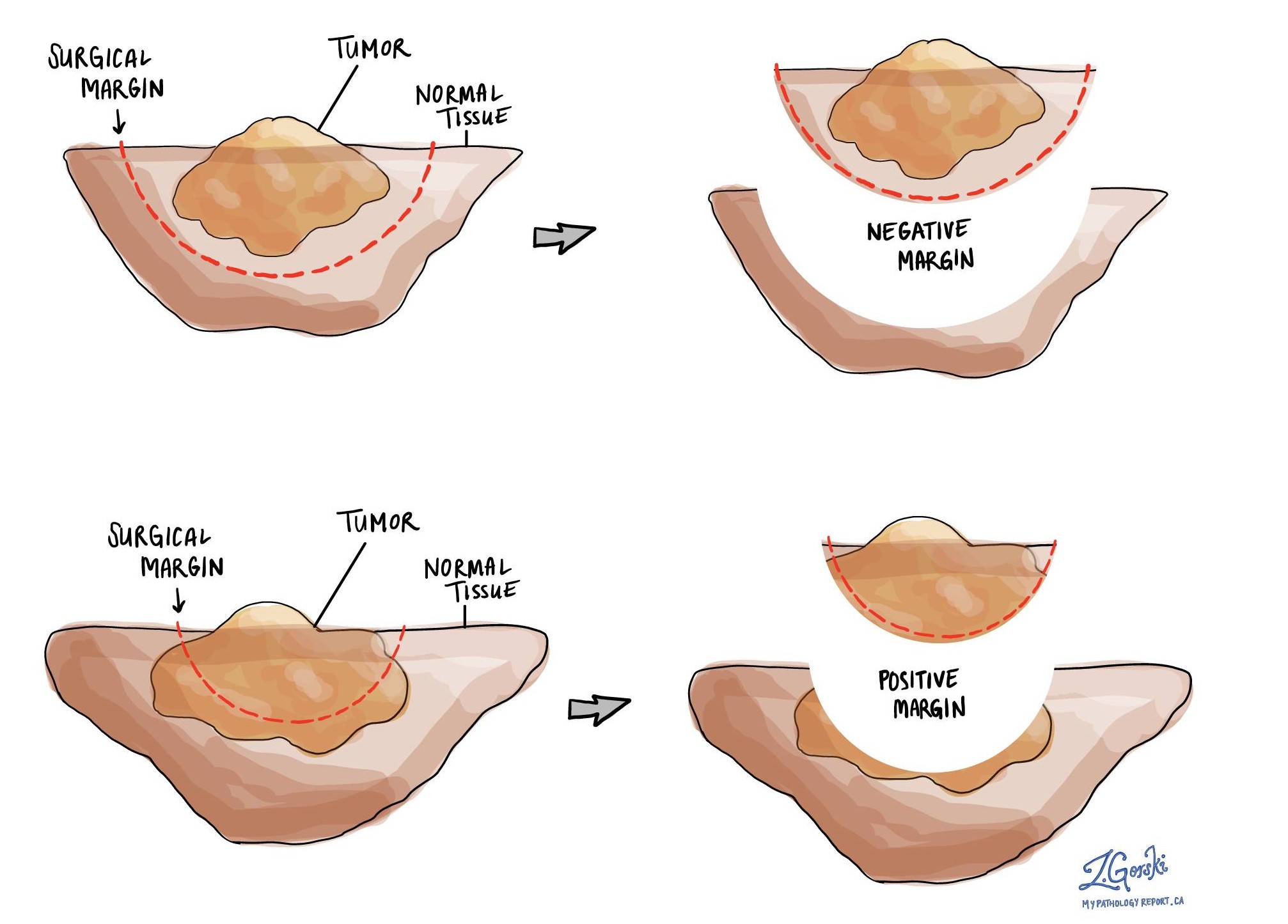
A margin is any tissue that was cut by the surgeon to remove the tumour from your body. Depending on the type of surgery you have had, the margins can include bones, muscles, blood vessels, and nerves that were cut to remove the tumour from your body.
A margin is called positive when there are tumour cells at the very edge of the cut tissue. A positive margin is associated with a higher risk that the tumour will recur in the same site after treatment. A negative margin means that no tumour cells were seen at any of the cut edges of tissue.
Molecular tests
Each cell in your body contains a set of instructions that tell the cell how to behave. These instructions are written in a language called DNA and the instructions are stored on 46 chromosomes in each cell. Because the instructions are very long, they are broken up into sections called genes and each gene tells the cell how to produce piece of the machine called a protein.
Sometimes, a piece of DNA falls off one chromosome and becomes attached to a different chromosome. This is called a translocation and it can result in the cell making a new and abnormal protein. Nodular fasciitis often contains a translocation that combines the gene MYH9 with the USP6 gene.
Pathologists can test for these molecular changes by performing molecular tests such as next-generation sequencing (NGS) on a piece of the tissue from the tumour. This type of testing is can be done on the biopsy specimen or when your tumor has been surgically removed.
In cases where nodular fasciitis has the typical appearance under the microscope, your pathologist most likely will not perform a molecular test to confirm the diagnosis.
We are proud to partner with:
![]()