

by Zuzanna Gorski MD FRCPC
March 2, 2026
Squamous cell carcinoma in situ, also called Bowen’s disease, is an early form of skin cancer.
It begins in squamous cells, which are flat cells that make up the outer layer of the skin, called the epidermis. In this condition, the squamous cells have become cancerous, but they are still confined to the epidermis.
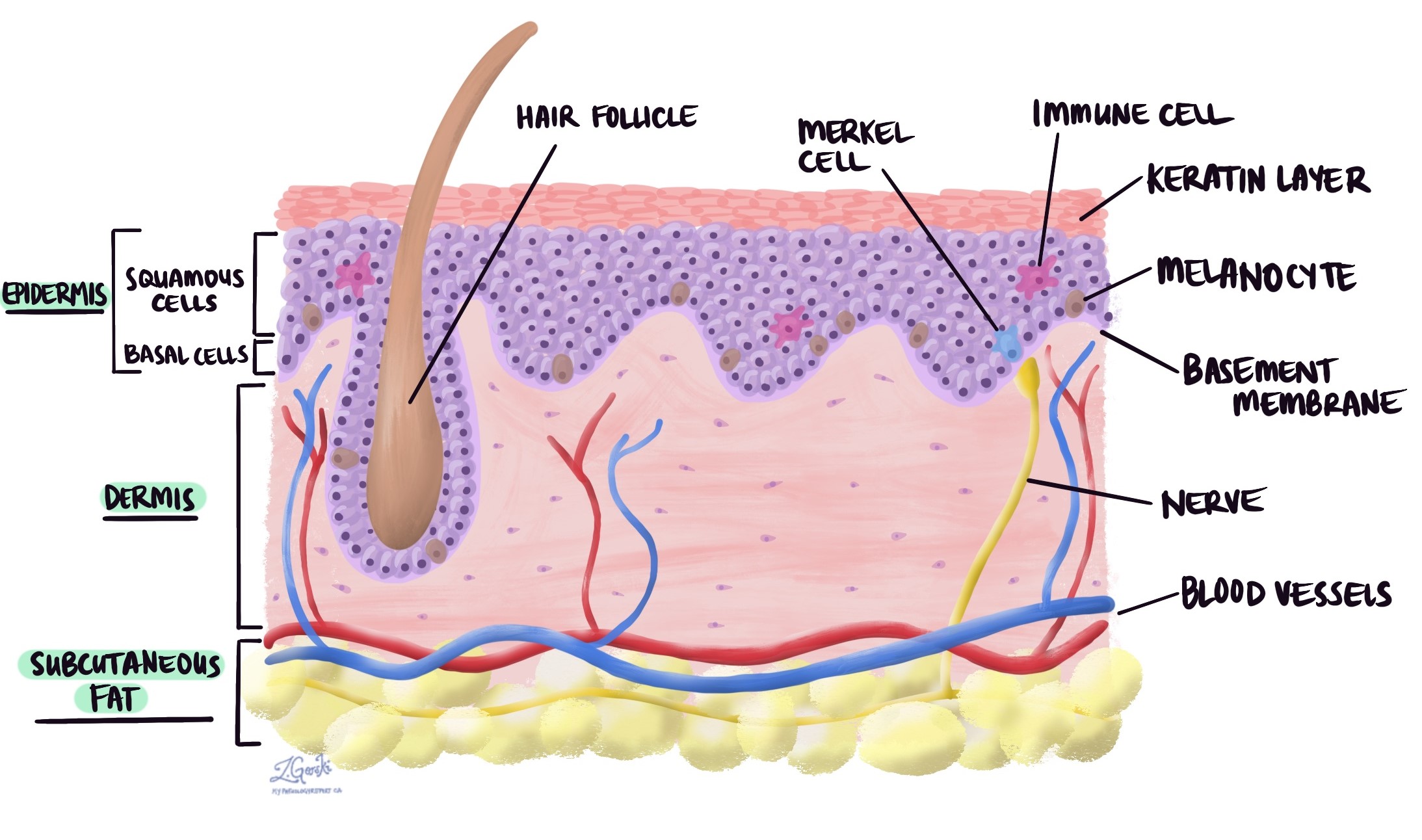
The term “in situ” means “in its original place.” This means that the abnormal cells have not grown into the deeper layer of skin, called the dermis. Because the cancer cells are limited to the epidermis, squamous cell carcinoma in situ is sometimes described as non-invasive squamous cell carcinoma.
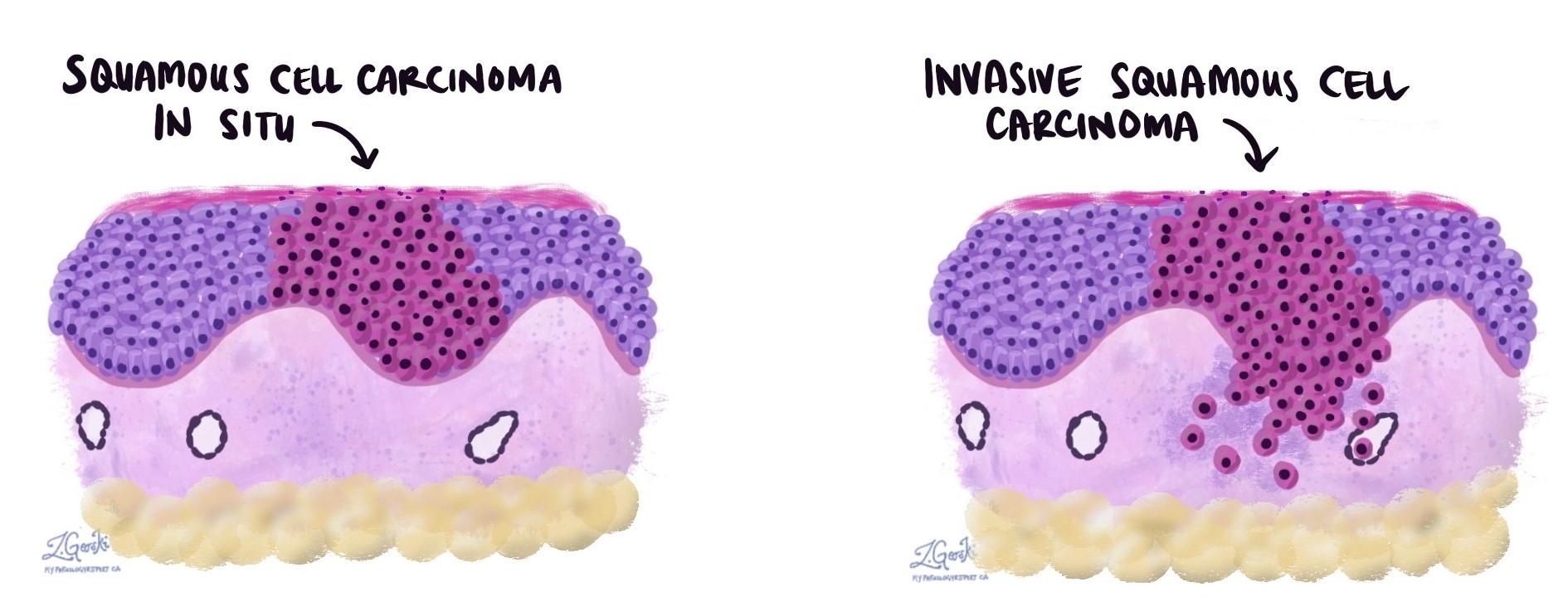
If left untreated, squamous cell carcinoma in situ can progress to invasive squamous cell carcinoma, which grows into deeper layers of the skin and may spread to other parts of the body.
What does squamous cell carcinoma in situ look like?
Squamous cell carcinoma in situ usually appears as a slow-growing, red or pink patch of skin. The surface is often dry, scaly, or crusted.
The lesion may feel rough to the touch and may be itchy, tender, or mildly sore. Because it can resemble other common skin conditions, such as eczema, psoriasis, or fungal infection, it is often diagnosed with a biopsy.
It most commonly develops on sun-exposed areas, including the face, neck, hands, and lower legs. However, it can occur anywhere on the skin.
What causes squamous cell carcinoma in situ?
The most common cause is long-term exposure to ultraviolet (UV) radiation, usually from sunlight. Artificial sources of UV radiation, such as tanning beds, also increase risk.
Other factors that increase risk include:
-
A weakened immune system, such as after an organ transplant or from immune-suppressing medications.
-
Chronic skin injury or inflammation.
-
Infection with certain types of human papillomavirus (HPV).
-
Older age.
Repeated UV exposure damages the DNA inside squamous cells. Over time, this damage can cause the cells to grow uncontrolled.
Is squamous cell carcinoma in situ cancer?
Yes. Squamous cell carcinoma in situ is made up of malignant (cancerous) cells. However, because the abnormal cells remain confined to the epidermis, they cannot spread to lymph nodes or distant parts of the body.
For this reason, when treated early, squamous cell carcinoma in situ is usually curable.
What is the risk of developing invasive squamous cell carcinoma?
If left untreated, squamous cell carcinoma in situ can develop into invasive squamous cell carcinoma. Studies suggest that this progression occurs in approximately 3–10% of cases.
The risk of progression is higher in immunosuppressed people, those with lesions on high-risk sites such as the lips or ears, or those who delay treatment for large or long-standing lesions.
Early treatment significantly reduces the risk of invasive cancer.
How is this diagnosis made?
The diagnosis is made after a biopsy, in which a small sample of the lesion is removed and examined under the microscope by a pathologist.
The pathologist confirms that the abnormal squamous cells are confined to the epidermis and have not invaded into the dermis. The biopsy also helps rule out other skin conditions that can look similar.
If the lesion is large, complete removal may be recommended to ensure that invasive cancer is not present.
Microscopic features
Under the microscope, squamous cell carcinoma in situ shows full-thickness abnormality of the epidermis.
The normal squamous cells are replaced by atypical cells that appear enlarged, dark-staining (hyperchromatic), and irregular in shape. The cells lose their normal orderly arrangement. Mitotic figures, which are cells actively dividing, are often increased.
Dyskeratotic cells, which are prematurely dying squamous cells, may be present. Importantly, the abnormal cells remain above the basement membrane and do not invade into the dermis.
If tumor cells are seen breaking through the basement membrane and growing into the dermis, the diagnosis changes to invasive squamous cell carcinoma.
Margins
A margin is the edge of the tissue removed during surgery. After the lesion is removed, the pathologist examines the margins under the microscope to determine whether abnormal cells extend to the cut edge.
A negative margin means that no cancer cells are seen at the edge of the tissue. This indicates that the lesion was completely excised, meaning it was fully removed.
A positive margin means that cancer cells are present at the edge of the tissue. This indicates that the lesion was incompletely excised, meaning that some abnormal cells may remain in the skin. In this situation, additional treatment is often recommended.
In some pathology reports, the distance between the cancer cells and the nearest margin is measured. A larger distance provides greater confidence that the lesion has been fully removed.
It is important to note that small diagnostic biopsies are not intended to remove the entire lesion. Therefore, positive margins are common in biopsy specimens. When a procedure is performed specifically to remove the lesion, the goal is complete excision with negative margins.
How is squamous cell carcinoma in situ treated?
Treatment options may include surgical excision, cryotherapy (freezing), topical medications, photodynamic therapy, or other dermatologic procedures. The choice of treatment depends on the size and location of the lesion and patient-specific factors.
Questions you may want to ask your doctor
-
Was the lesion completely removed?
-
Were the margins negative?
-
What is my risk of progression to invasive cancer?
-
Do I need additional treatment?
-
How often should I have follow-up skin examinations?
-
What signs should I watch for that might suggest recurrence?
We are proud to partner with:
![]()