

by Jason Wasserman MD PhD FRCPC
April 28, 2026
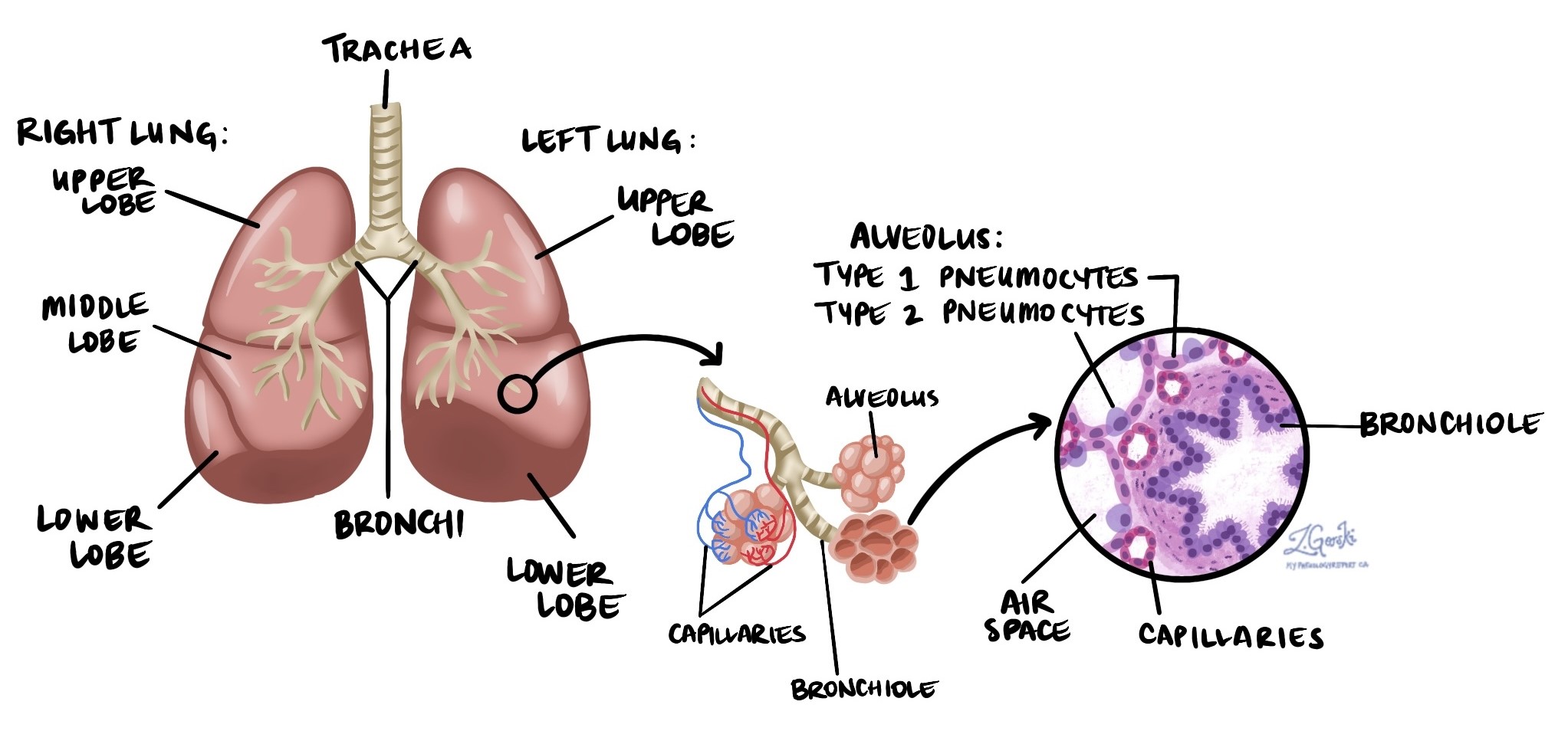
Adenocarcinoma in situ (AIS) is a type of early, non-invasive lung cancer. Non-invasive means the cancer cells have not grown beyond the inner lining of the tiny air sacs — called alveoli — that make up the lung. By definition, a tumor must be no larger than 3 centimeters to be classified as adenocarcinoma in situ. When completely removed by surgery, AIS is associated with an excellent outcome. This article will help you understand the findings in your pathology report — what each term means and why it matters for your care.
What causes adenocarcinoma in situ?
The primary cause of adenocarcinoma in situ in the lung is tobacco smoking. Smoking exposes the lungs to harmful chemicals that can damage the DNA inside lung cells and lead to cancerous changes over time. However, AIS also occurs in people who have never smoked.
Other risk factors include:
- Radon gas exposure — Radon is a naturally occurring radioactive gas that can accumulate in homes and buildings. Long-term exposure is a recognized risk factor for lung cancer.
- Occupational exposures — Prolonged contact with substances such as asbestos, silica dust, or diesel exhaust in certain workplaces may contribute to the development of lung cancer.
- Air pollution — Long-term exposure to outdoor air pollution is associated with a modestly increased risk of lung cancer.
What are the symptoms of adenocarcinoma in situ?
Adenocarcinoma in situ almost never causes symptoms. Because the tumor is small and has not grown into the surrounding lung tissue or beyond, it does not obstruct airways or irritate nearby structures. Most cases are discovered incidentally — found by chance on imaging such as a chest X-ray or CT scan performed for an unrelated reason, or identified during lung cancer screening.
Is adenocarcinoma in situ a type of cancer?
Yes, adenocarcinoma in situ is classified as a type of lung cancer — specifically, a non-invasive one. “In situ” is a Latin phrase meaning “in place,” and it indicates that the cancer cells are confined to the inner lining of the alveoli and have not broken through into the surrounding lung tissue. The cancer cells in AIS look very similar to those found in invasive adenocarcinoma of the lung, but they behave very differently: unlike invasive adenocarcinoma, AIS does not spread into surrounding tissue, enter blood or lymphatic vessels, or metastasize to lymph nodes or other organs.
If left untreated, adenocarcinoma in situ can eventually progress to invasive adenocarcinoma — a cancer that does spread into surrounding lung tissue and carries a higher risk of recurrence and spread to other parts of the body. Complete surgical removal prevents this progression.
How is the diagnosis made?
The diagnosis of adenocarcinoma in situ is almost always made after the entire tumor has been surgically removed and examined in full by a pathologist — a doctor who specializes in diagnosing disease by examining tissue under the microscope. This is a critical point: adenocarcinoma in situ cannot be reliably diagnosed from a small biopsy sample, because a biopsy captures only a small portion of the tumor and cannot confirm that no invasive growth is present elsewhere. A pre-surgical biopsy may raise suspicion for AIS or early adenocarcinoma, but the definitive diagnosis requires examination of the complete specimen.
On imaging, AIS typically appears as a ground-glass opacity — a hazy, faintly cloudy area on a CT scan that does not completely block out the underlying lung structure. This appearance reflects the fact that the tumor cells grow along the surface of the alveoli without filling them in or collapsing them. A pure ground-glass nodule with no solid component is characteristic of AIS, though imaging alone cannot confirm the diagnosis.
Under the microscope, the pathologist confirms AIS by identifying a specific growth pattern called lepidic growth — a pattern in which cancer cells spread along the inner surface of the alveoli like a thin coating, without invading the underlying tissue framework. The cancer cells look larger, darker, and more irregular than normal lung lining cells, but they remain strictly confined to the alveolar surface. To confirm the diagnosis, the pathologist must examine the entire tumor and verify that there is no area of stromal invasion — meaning no cancer cells have broken through the alveolar lining and grown into the supporting tissue of the lung — and that the tumor measures 3 centimeters or less in its greatest dimension. Immunohistochemistry stains may be used to confirm that the cells are of lung origin (typically TTF-1 positive) and to help distinguish AIS from other conditions that can mimic it, such as atypical adenomatous hyperplasia or reactive pneumocyte changes.
Once the diagnosis is confirmed, your doctor may recommend follow-up CT imaging to monitor the remaining lung tissue for the development of additional lesions.
Histologic grade
Adenocarcinoma in situ is not assigned a histologic grade. Grading describes how aggressive an invasive cancer appears under the microscope and is based on features such as the predominant growth pattern and the degree of cellular abnormality. Because AIS is by definition non-invasive — the cancer cells have not grown into the surrounding lung tissue — the grading system used for invasive lung adenocarcinoma does not apply. The diagnosis of AIS itself carries an excellent prognosis when the tumor is completely removed.
What is the difference between adenocarcinoma in situ and minimally invasive adenocarcinoma?
Adenocarcinoma in situ and minimally invasive adenocarcinoma (MIA) are both very early forms of lung adenocarcinoma, and both carry an excellent prognosis with complete surgical removal. The key difference is whether any invasion into the surrounding lung tissue has occurred.
- Adenocarcinoma in situ — The tumor shows pure lepidic growth with no invasion whatsoever into the surrounding lung tissue. The tumor is 3 centimeters or smaller. There is no risk of spread to lymph nodes or distant organs.
- Minimally invasive adenocarcinoma — The tumor is predominantly lepidic but contains a small focus of stromal invasion — meaning a tiny area (5 millimeters or less) where cancer cells have broken through the alveolar lining and grown into the surrounding tissue. The tumor is still 3 centimeters or smaller overall.
This distinction is made by the pathologist after carefully measuring any invasive component throughout the entire tumor. Both diagnoses are associated with near-100% disease-specific survival after complete resection, but the presence of even minimal invasion means MIA requires somewhat closer monitoring than pure AIS.
Pathologic stage
Adenocarcinoma in situ is classified as pTis in the pathologic staging system — the “is” stands for “in situ.” This corresponds to Stage 0, the earliest possible stage in the cancer staging system. Stage 0 means the cancer is entirely confined to the inner lining of the alveoli, with no invasion into surrounding lung tissue, no spread to lymph nodes, and no distant metastasis. Because these features are definitional for AIS — a tumor cannot be classified as AIS if any of them are present — all cases of adenocarcinoma in situ are Stage 0 by definition.
What is the prognosis?
The prognosis for adenocarcinoma in situ is excellent. When the tumor is completely removed by surgery with clear margins, the disease-specific five-year survival rate is essentially 100% — meaning that virtually no patients die from AIS itself after successful resection. Because AIS does not invade surrounding tissue and does not spread to lymph nodes or other organs, it behaves more like a curable localized lesion than a conventional cancer.
The most important prognostic factors are:
- Complete surgical removal — The single most important factor. A negative surgical margin — meaning no cancer cells at the cut edges of the removed tissue — confirms that the tumor has been fully excised. If the margin is positive or very close, further surgery may be recommended.
- Absence of invasion — Confirmation that no area of stromal invasion is present throughout the entire tumor is required to maintain the AIS diagnosis and its favorable prognosis.
- Risk of additional lung tumors — Patients who have had AIS are at a modestly increased risk of developing additional synchronous (occurring at the same time) or metachronous (occurring later) lung tumors, which is why ongoing surveillance imaging is recommended after treatment.
What happens after the diagnosis?
Because adenocarcinoma in situ is non-invasive and does not spread, surgery to completely remove the tumor is the only treatment needed in the vast majority of cases. Chemotherapy and radiation therapy are not indicated for AIS.
The type of surgery depends on the size and location of the tumor and the patient’s overall lung function. For small, peripheral tumors, a wedge resection — in which a wedge-shaped segment of lung tissue containing the tumor is removed — is usually sufficient. For larger tumors or those in less accessible locations, a segmentectomy (removal of a defined segment of lung) or lobectomy (removal of an entire lobe) may be preferred to ensure complete removal with adequate margins. The choice of surgical approach is made by a thoracic surgeon in consultation with the broader care team.
After surgery, regular follow-up is important. Annual chest CT imaging is typically recommended to monitor the remaining lung for new ground-glass nodules or other abnormalities. The duration and frequency of follow-up will be determined by your care team based on your individual situation. Because AIS is associated with tobacco smoking, smoking cessation — if applicable — is strongly encouraged and has been shown to reduce the risk of developing additional lung tumors.
Questions to ask your doctor
- Was the adenocarcinoma in situ completely removed, and what were the surgical margins?
- Did the pathologist find any area of invasion in the tumor, or is it confirmed to be purely in situ?
- What is the difference between adenocarcinoma in situ and minimally invasive adenocarcinoma, and which diagnosis applies to me?
- How large was the tumor, and does the size affect my risk of recurrence?
- What type of surgery was performed, and was it the most appropriate approach for my tumor?
- Do I need any additional treatments after surgery?
- What follow-up imaging schedule do you recommend, and for how long?
- What symptoms should prompt me to contact you between scheduled visits?
- Am I at increased risk of developing additional lung tumors, and what can I do to reduce that risk?
- Should I be referred for lung cancer screening going forward, and what does that involve?
- Does smoking cessation affect my risk of a new lung tumor, and can you connect me with resources to help?
We are proud to partner with:
![]()