

Jason Wasserman MD PhD FRCPC
November 19, 2023
Phyllodes tumour is a rare type of breast tumour. Most phyllodes tumours will behave like non-cancerous tumours. However, a small number (approximately 10%) will behave like cancer. This behaviour includes the ability to spread through the normal tissue in the breast and to other parts of the body. The entire tumour must be removed surgically before your pathologist can decide if the tumour is a non-cancerous or cancerous type of phyllodes tumour.
What are the symptoms of a phyllodes tumour?
Phyllodes tumours usually present as a round, painless lump that you or your doctor can feel during an examination of the breasts. These tumours tend to grow quickly which may cause the skin on top of the tumour to stretch. Most tumours measure several centimetres by the time they are removed.
How is this diagnosis made?
The diagnosis of a phyllodes tumour can be made after a small tissue sample is removed in a procedure called a biopsy. However, the biopsy may not provide enough tissue for your pathologist to decide if the tumour is benign, borderline, or malignant.
About this article
This article was written by doctors to help you read and understand your pathology report for phyllodes tumour. The sections below describe the results found in most pathology reports, however, all reports are different and results may vary. Importantly, some of this information will only be described in your report after the entire tumour has been surgically removed and examined by a pathologist. Contact us if you have any questions about this article or your pathology report. Read this article for a more general introduction to the parts of a typical pathology report.
What does a phyllodes tumour look like under the microscope?
A phyllodes tumour starts from the cells normally found in the breast. The tumour is made up of a mixture of fibroblasts surrounded by stroma and epithelial cells which form large ducts. When examined under the microscope, the tumour often grows in a pattern resembling a tree’s leaves. This pattern can be helpful for pathologists when examining only a small tissue sample. The name “phyllodes” comes from the Greek meaning ‘leaf-like’.

What is the difference between a benign, borderline, and malignant phyllodes tumour?
Pathologists divide phyllodes tumours into three types – benign, borderline, and malignant – based on the way the tumour looks when examined under the microscope. The type of tumour will help your doctor predict how the tumour will behave over time and select treatment options that are right for you.
Benign phyllodes tumour?
A benign phyllodes tumour is a non-cancerous tumour. When examined under the microscope these tumours show no features of cancer. These tumours are usually treated with surgery alone. The tumour may grow back after surgery if the tumour is not completely removed.
Borderline phyllodes tumour?
When examined under the microscope, a borderline phyllodes tumour has features that can be seen in both non-cancerous tumours and cancers. For this reason, a borderline tumour falls in between benign and malignant. Treatment for this type of tumour depends on the number of worrisome features seen. Most are treated with surgery alone, but some patients may be offered radiation therapy. The tumour may grow back after surgery if it is not completely removed.
Malignant phyllodes tumour?
A malignant phyllodes tumour is considered a type of cancer. Like other types of cancer, the tumour cells in a malignant phyllodes tumour can metastasize (spread) to other parts of the body. Additional treatment such as radiation or chemotherapy may be required for a malignant phyllodes tumour.
How do pathologists decide if a phyllodes tumour is benign, borderline, or malignant?
When examining the tumour under the microscope, pathologists look for several features to determine if the tumour is benign, borderline, or malignant. These microscopic features include stromal cellularity, stromal overgrowth, cellular atypia, mitotic activity, and an infiltrative pattern of growth. These features are described in greater detail in the sections below.
Stromal cellularity
Stroma is the connective tissue that surrounds the ducts and glands in the breast. Most of the stroma is made up of cells called fibroblasts. Stromal cellularity is a term pathologists use to describe the number of fibroblasts within the stroma. Benign tumours have the least number of fibroblasts while malignant tumours have the most.
Stromal overgrowth
Stromal overgrowth is used to describe a tumour that has areas made up entirely of stroma with no epithelial cells. Stromal overgrowth is not seen in a benign tumour. Small areas of stromal overgrowth can be seen in a borderline tumour while large areas of stromal overgrowth are common in malignant tumours.
Atypia
Atypia is a word pathologists use to describe cells that look different from normal, healthy cells in that same location. Pathologists look at the size, shape, and colour of the cells to decide if they are atypical.
The cells in a benign phyllodes tumour are like those found in normal, healthy breast tissue. The cells in a borderline phyllodes tumour are atypical although they still share some features with normal, healthy cells. In contrast, the cells in a malignant phyllodes tumour are typically much larger, darker, and have irregular shapes compared to normal, healthy cells. Pathologists describe these cells as showing marked or significant cytologic atypia.
Mitotic activity
Cells divide to create new cells. The process of creating a new cell is called mitosis, and a cell that is dividing is called a mitotic figure. The number of dividing cells is an important feature for the pathologist to count when determining the type of phyllodes tumour. For this reason, many pathology reports will include the number of mitotic figures seen in the tissue sample. The count is usually expressed as the number of mitotic figures seen in 10 high-power (high magnification) microscopic fields examined.
Pathologists use established criteria for determining if the number of mitotic figures is consistent with a benign, borderline, or malignant phyllodes tumour. The criteria are as follows:
- Benign – Less than 5 mitotic figures per 10 high-powered fields.
- Borderline – 5 to 9 mitotic figures per 10 high-powered fields.
- Malignant – 10 or more mitotic figures per 10 high-powered fields.
Tumour margin
The tumour margin is the part of the tumour that touches the surrounding normal breast tissue. The margin between the tumour and the surrounding normal breast tissue is an important feature that helps your pathologist decide if the tumour is benign, borderline, or malignant.
- Benign – The tumour margin is clear, easy to see, and well-separated from the surrounding normal breast tissue.
- Borderline – The tumour margin is mostly clear and easy to see although in some areas the tumour extends into the normal breast tissue in a way that makes it difficult to see the border.
- Malignant – The tumour spreads into the surrounding normal breast tissue in a way that makes it very difficult for your pathologist to see the tumour margin. Pathologists describe this as an infiltrative pattern of growth.
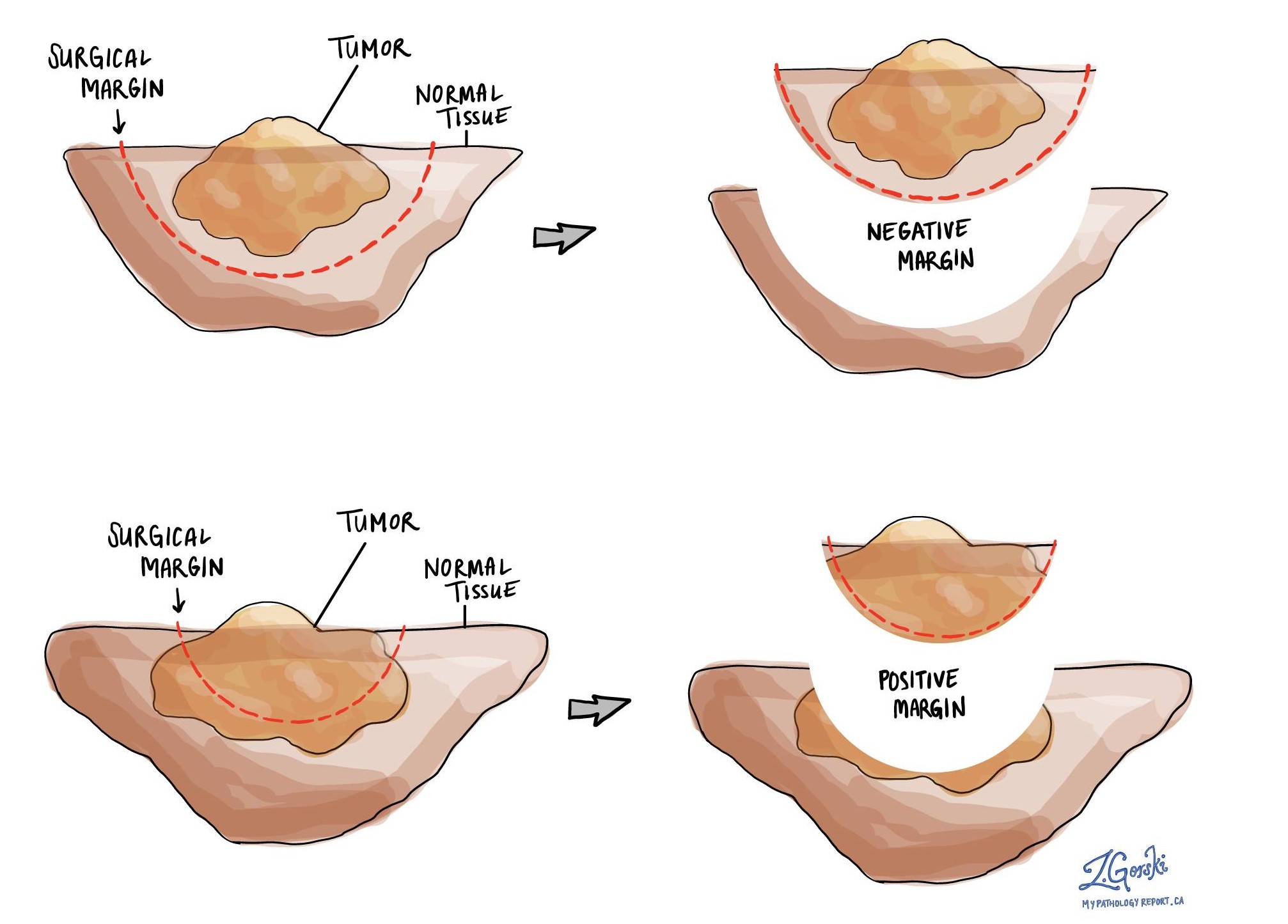
What is a surgical margin and why is it important?
In pathology, a surgical margin is the edge of a tissue that is cut when removing a tumour from the body. The margins described in a pathology report are very important because they tell you if the entire tumour was removed or if some of the tumour was left behind. The margin status will determine what (if any) additional treatment you may require. For phyllodes tumours, a surgical resection margin of at least 1 cm is recommended to reduce the chance that the tumour will regrow after surgery.
Most pathology reports only describe margins after a surgical procedure called an excision or resection has been performed to remove the entire tumour. For this reason, margins are not usually described after a procedure called a biopsy is performed to remove only part of the tumour. The number of margins described in a pathology report depends on the types of tissues removed and the location of the tumour. The size of the margin (the amount of normal tissue between the tumour and the cut edge) depends on the type of tumour being removed and the location of the tumour.
Pathologists carefully examine the margins to look for tumour cells at the cut edge of the tissue. If tumour cells are seen at the cut edge of the tissue, the margin will be described as positive. If no tumour cells are seen at the cut edge of the tissue, a margin will be described as negative. Even if all of the margins are negative, some pathology reports will also provide a measurement of the closest tumour cells to the cut edge of the tissue.
A positive (or very close) margin is important because it means that tumour cells may have been left behind in your body when the tumour was surgically removed. For this reason, patients who have a positive margin may be offered another surgery to remove the rest of the tumour or radiation therapy to the area of the body with the positive margin. The decision to offer additional treatment and the type of treatment options offered will depend on a variety of factors including the type of tumour removed and the area of the body involved. For example, additional treatment may not be necessary for a benign (non-cancerous) type of tumour but may be strongly advised for a malignant (cancerous) type of tumour.
Other helpful resources
Atlas of Pathology
We are proud to partner with:
![]()