

by Jason Wasserman MD PhD FRCPC
November 19, 2025
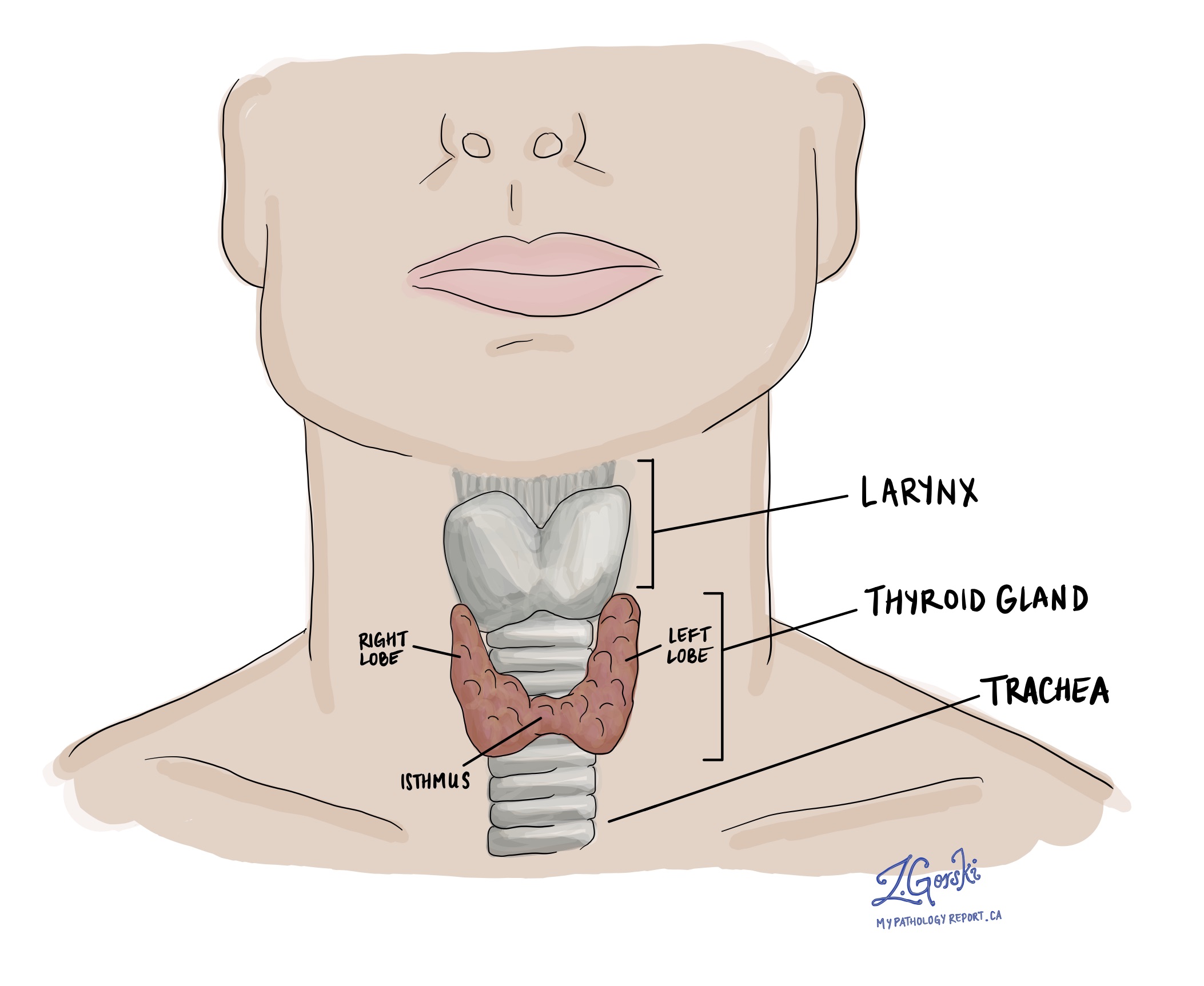
Follicular variant papillary thyroid carcinoma is a type of thyroid cancer and a subtype of papillary thyroid carcinoma, the most common thyroid cancer. It develops from follicular cells, which are the thyroid cells responsible for producing thyroid hormone.
The tumour is called a “follicular variant” because, under the microscope, the cancer cells exhibit a follicular growth pattern, forming tiny circular structures resembling normal thyroid follicles. At the same time, they demonstrate the nuclear features of papillary thyroid carcinoma, including enlarged, pale nuclei with grooves or overlapping edges. These nuclear changes help the pathologist identify the tumour as part of the papillary thyroid carcinoma family.
Follicular variant papillary thyroid carcinoma often behaves differently from classic papillary thyroid carcinoma. Many cases are less aggressive, particularly when the tumour is encapsulated and shows only minimal invasion. However, some subtypes are more aggressive, so the microscopic pattern plays an important role in predicting behaviour and selecting the proper treatment.
What are the symptoms of follicular variant papillary thyroid carcinoma?
Many people with follicular variant papillary thyroid carcinoma have no symptoms, and the tumour is detected when a nodule is found on examination or ultrasound. When symptoms do occur, they are similar to those of other thyroid cancers. They can include a palpable nodule or lump in the neck, neck swelling, hoarseness or changes in voice, difficulty swallowing, difficulty breathing, or a persistent cough not related to a cold.
What causes follicular variant papillary thyroid carcinoma?
The exact cause of follicular variant papillary thyroid carcinoma is not fully understood. As with other thyroid cancers, it likely results from a combination of genetic changes and environmental risk factors.
Previous exposure to radiation, especially during childhood, increases the risk of developing this tumour. Follicular variant papillary thyroid carcinoma is often associated with mutations in the RAS family of genes. Only a minority of cases show BRAF gene mutations, which are more commonly seen in the classic subtype of papillary thyroid carcinoma. These genetic changes alter how thyroid cells grow and divide, allowing them to form a malignant tumour.
How is this diagnosis made?
Diagnosing follicular variant papillary thyroid carcinoma requires a combination of imaging, biopsy, and microscopic examination. Because the tumour grows in follicular patterns, the final diagnosis usually cannot be confirmed until the entire nodule is removed and examined under a microscope by a pathologist.
Clinical examination and ultrasound
The process usually begins when a thyroid nodule is found during a physical exam. Ultrasound is then used to evaluate the nodule’s size, shape, and internal features. Some ultrasound characteristics may suggest malignancy, but ultrasound alone cannot determine the subtype of cancer.
Fine needle aspiration (FNA)
A fine needle aspiration removes cells from the nodule for microscopic examination. While FNA is excellent for diagnosing many thyroid cancers, it often cannot distinguish between:
-
Benign follicular nodules.
-
Follicular adenoma.
-
Follicular variant papillary thyroid carcinoma.
This is because the important features used to diagnose follicular variant papillary thyroid carcinoma—capsular invasion (cancer breaking through the tumour capsule) and vascular invasion (cancer cells entering blood vessels)—cannot be assessed on small FNA samples.
Surgical removal
A final diagnosis usually requires surgery to remove part or all of the thyroid gland. The nodule, surrounding capsule, and nearby thyroid tissue must be examined under the microscope.
Microscopic examination
The pathologist examines the surgically removed tumour and looks for:
-
The nuclear features of papillary thyroid carcinoma.
-
A follicular growth pattern.
-
Capsular invasion, meaning tumour cells are breaking through the tumour capsule.
-
Vascular invasion, meaning tumour cells are present inside nearby blood vessels.
These features confirm the diagnosis and determine the tumour subtype.
Subtypes of follicular variant papillary thyroid carcinoma
After microscopic examination, follicular variant papillary thyroid carcinoma can be categorized into different subtypes based on how the tumour grows and invades surrounding tissue. These subtypes help predict how the tumour will behave and may influence treatment decisions.
Minimally invasive encapsulated follicular variant papillary thyroid carcinoma
In this subtype, the tumour is surrounded by a fibrous capsule. Under the microscope, only limited invasion through the capsule or into nearby thyroid tissue is seen. This subtype is usually associated with an excellent prognosis and a low risk of metastasis compared to widely invasive or angioinvasive tumours.
Widely invasive follicular variant papillary thyroid carcinoma
In widely invasive tumours, cancer cells extensively invade surrounding thyroid tissue beyond the capsule. Vascular invasion may or may not be present. This subtype is more aggressive and has a higher risk of distant spread and recurrence than minimally invasive tumours.
Encapsulated angioinvasive follicular variant papillary thyroid carcinoma
This subtype has a well-defined capsule and shows vascular invasion but limited or no capsular invasion. It falls between minimally invasive and widely invasive tumours in terms of aggressiveness and prognosis. The extent of vascular invasion is particularly important in this subtype.
Tumour size
Once the tumour has been completely removed, it is measured in three dimensions. The largest dimension is recorded in the pathology report. For example, a tumour that measures 4.0 cm by 2.0 cm by 1.5 cm will be reported as 4.0 cm.
Tumour size is important because it is used to determine the pathologic tumour stage (pT). Larger tumours are more likely to spread outside the thyroid or to lymph nodes and may require more intensive treatment and follow-up.
Extrathyroidal extension
Extrathyroidal extension means that cancer cells have spread outside the thyroid gland into surrounding tissues. It is an important factor in staging and prognosis.
Microscopic extrathyroidal extension
Microscopic extension is seen only under the microscope and indicates minimal spread through the thyroid capsule into nearby soft tissues.
Macroscopic (gross) extrathyroidal extension
Macroscopic extension is visible to the surgeon during the operation or on imaging. It involves an obvious invasion of neighbouring structures, such as the neck muscles, trachea, esophagus, or major blood vessels.
Macroscopic extrathyroidal extension is associated with a worse prognosis, a higher tumour stage, and may lead to more aggressive treatment and closer follow-up.
Vascular invasion (angioinvasion)
Vascular invasion, also called angioinvasion, means cancer cells are found inside blood vessels in or around the tumour. This is an important feature because it increases the risk that cancer cells will spread to distant sites such as the lungs or bones.
Pathologists describe vascular invasion as:
-
Focal vascular invasion, when cancer cells are found in fewer than 4 blood vessels.
-
Extensive vascular invasion, when cancer cells are found in 4 or more blood vessels.
Extensive vascular invasion is associated with a higher risk of metastasis and a worse prognosis. When extensive vascular invasion is present, doctors may recommend more aggressive treatment and closer monitoring.
Lymphatic invasion
Lymphatic invasion means cancer cells have entered lymphatic channels, which are small vessels that carry lymph fluid to lymph nodes. In follicular variant papillary thyroid carcinoma, lymphatic invasion is less common than in classic papillary thyroid carcinoma and is not always associated with a more aggressive course. Nonetheless, it is reported because it indicates that tumour cells have access to the lymphatic system and may travel to lymph nodes.
Margins
Margins are the edges of the tissue removed during surgery. The pathologist examines these edges under the microscope to see whether cancer cells are present.
-
A negative margin means no cancer cells are seen at the cut edge, suggesting that the tumour has been completely removed.
-
A positive margin means cancer cells are present at the edge, indicating that some tumour may remain.
Sometimes the pathologist also measures the distance between the tumour and the closest margin. Margin status helps determine whether additional treatment, such as radioactive iodine or further surgery, may be needed.
Lymph nodes
Lymph nodes are small immune organs that filter lymph fluid and trap abnormal cells, including cancer cells. Cancer can spread from the thyroid to lymph nodes via lymphatic vessels.
In follicular variant papillary thyroid carcinoma, spread to lymph nodes is less common than in classic papillary thyroid carcinoma, but it can still occur, particularly in more aggressive subtypes.
Neck dissection and lymph node assessment
A neck dissection may be performed to remove lymph nodes from one or both sides of the neck. Lymph nodes are grouped into anatomical levels (1 through 5). Lymph nodes on the same side as the tumour are called ipsilateral, and those on the opposite side are called contralateral.
The pathologist examines each lymph node and reports:
-
The number of lymph nodes examined.
-
The number that contain cancer (positive nodes).
-
The size of the largest tumour deposit.
-
Whether extranodal extension is present, meaning tumour cells have grown through the lymph node capsule into the surrounding tissue.
Lymph node involvement is used to determine the nodal stage (pN) and helps guide decisions on additional treatment and follow-up.
Biomarkers for follicular variant papillary thyroid carcinoma
Follicular variant papillary thyroid carcinoma is often associated with specific genetic changes. Identifying these changes can help confirm the diagnosis and may provide information about tumour behaviour.
Types of biomarker testing
Biomarkers are usually assessed using tumour tissue and may include:
-
Next-generation sequencing (NGS) or PCR to detect point mutations in RAS or BRAF.
-
FISH to detect gene rearrangements.
-
Immunohistochemistry (IHC) in select cases to support the diagnosis or identify protein expression patterns related to underlying genetic changes.
Results are typically reported by listing the specific gene and mutation or rearrangement detected.
RAS mutations
Follicular variant papillary thyroid carcinoma frequently harbours mutations in the RAS gene family (HRAS, KRAS, NRAS). These mutations activate growth pathways and are more common in follicular-patterned tumours. RAS mutations may be associated with a more indolent course compared to BRAF-mutated classic papillary thyroid carcinoma.
BRAF mutations
BRAF mutations, particularly BRAF V600E, are common in classic papillary thyroid carcinoma but are seen in only a minority of follicular variant cases. When present, BRAF mutations may be associated with more aggressive behaviour. The absence of BRAF mutations in many follicular variant tumours is one reason this variant is sometimes associated with a more favourable prognosis.
How is follicular variant papillary thyroid carcinoma different from classic papillary thyroid carcinoma?
Both follicular variant and classic papillary thyroid carcinoma are types of papillary thyroid carcinoma, but they differ in microscopic appearance, patterns of spread, and often in prognosis.
Microscopic appearance
-
Follicular variant: Tumour cells have the nuclear features of papillary thyroid carcinoma (nuclear grooves, inclusions, and overlapping) but are arranged in small follicles. Papillary structures are absent or minimal.
-
Classic variant: Tumour cells form true papillary structures with fibrovascular cores. Nuclear features of papillary thyroid carcinoma are prominent, and calcified structures called psammoma bodies are commonly seen.
Behaviour
Follicular variant papillary thyroid carcinoma, especially the minimally invasive encapsulated subtype, generally has a better prognosis and is less likely to spread to lymph nodes compared with the classic variant. The classic variant more frequently spreads to cervical lymph nodes and may be more aggressive in some patients.
Prognosis
The overall prognosis for patients with follicular variant papillary thyroid carcinoma is generally very good. Most patients have an excellent outcome with appropriate treatment, typically surgery with or without radioactive iodine therapy. The five-year survival rate is over 95 percent.
Several pathologic features can influence prognosis:
-
Tumour size: Smaller tumours (less than 4 cm) are associated with a better outcome. Larger tumours have a higher risk of spread.
-
Extrathyroidal extension: Tumours that grow beyond the thyroid capsule into surrounding tissues are more likely to recur and spread.
-
Vascular invasion: The presence of cancer cells in blood vessels increases the risk of spread to distant sites such as the lungs or bones.
-
Lymph node involvement: Spread to lymph nodes can affect prognosis, although many patients still do very well with appropriate treatment.
-
Histologic subtype: Minimally invasive encapsulated tumours have an excellent prognosis. Widely invasive or angioinvasive subtypes show more aggressive behaviour and may require more intensive treatment and follow-up.
-
BRAF mutation status: The absence of BRAF mutations, which are common in classic papillary thyroid carcinoma, may be associated with a more favourable prognosis in follicular variant cases.
What happens after the diagnosis?
After a diagnosis of follicular variant papillary thyroid carcinoma is made, your healthcare team will review your pathology report, imaging results, thyroid function tests, and overall health to create a personalized treatment plan. This team may include an endocrinologist, a thyroid surgeon, a radiation oncologist, a nuclear medicine specialist, and, sometimes, a medical oncologist.
Most patients are treated with surgery, either a lobectomy (removal of one lobe) or a total thyroidectomy (removal of the entire thyroid gland). The type of surgery depends on tumour size, subtype, presence of vascular invasion or extrathyroidal extension, and whether lymph nodes are involved.
After surgery, some patients may receive radioactive iodine therapy, especially when there is a higher risk of recurrence or when extensive vascular invasion or lymph node involvement is present. Radioactive iodine helps destroy any remaining thyroid tissue or microscopic cancer cells.
Most patients will take thyroid hormone replacement after surgery. This medication both replaces the thyroid hormone your body can no longer make and reduces the chance of cancer recurrence by lowering thyroid-stimulating hormone (TSH) levels.
Your team will schedule regular follow-up visits. Follow-up may include blood tests (such as thyroglobulin levels, when appropriate), physical examinations, and neck ultrasounds to monitor for recurrence. Additional imaging or treatment may be recommended depending on your pathology features and response to initial therapy.
Questions for your doctor
-
What subtype of follicular variant papillary thyroid carcinoma do I have, and how does it affect my treatment?
-
Did my tumour show vascular invasion, lymphatic invasion, or extrathyroidal extension?
-
Were the surgical margins free of cancer?
-
Was more than one tumour found (multifocal disease)?
-
Were any lymph nodes involved, and was extranodal extension present?
-
What is my pathologic stage (pT and pN)?
-
Did my tumour show genetic changes such as RAS or BRAF mutations?
-
Do I need radioactive iodine treatment after surgery?
-
Will I need lifelong thyroid hormone replacement?
-
How often will I need follow-up appointments, blood tests, and imaging?
-
What signs or symptoms should prompt me to seek medical attention between follow-ups?
We are proud to partner with:
![]()