

by Jason Wasserman MD PhD FRCPC and Kamran M. Mirza MBBS PhD
October 21, 2025
Monoclonal gammopathy of undetermined significance (MGUS) is a condition in which abnormal plasma cells in the bone marrow make a small amount of a single type of antibody, called a monoclonal protein or M-protein.
MGUS is not necessarily cancer, but it is considered a precursor (early stage) in the spectrum of plasma cell disorders. It can remain stable for many years and often causes no symptoms or organ damage. However, a small number of people with MGUS will eventually develop a plasma cell cancer such as multiple myeloma, Waldenström macroglobulinemia, or amyloidosis.
Pathologists diagnose MGUS by combining blood test results, urine studies, and sometimes a bone marrow biopsy.
What causes monoclonal gammopathy of undetermined significance?
The exact cause of MGUS is not known. It develops when a single plasma cell in the bone marrow begins to grow and divide more than normal, producing one type of antibody in excess. The abnormal plasma cells do not invade bone or organs, and the total amount of M-protein they make remains low.
MGUS is more common in older adults, in men, and in people of African ancestry. A family history of plasma cell disorders such as multiple myeloma or amyloidosis slightly increases the risk.
What are the symptoms of monoclonal gammopathy of undetermined significance?
Most people with MGUS have no symptoms, and the condition is often discovered by accident during blood tests done for other reasons.
Because MGUS does not cause organ damage, the usual features seen in multiple myeloma—such as bone pain, anemia, kidney problems, or high calcium—are not present. However, ongoing monitoring is important to ensure that MGUS does not progress to a more serious condition over time.
How is monoclonal gammopathy of undetermined significance diagnosed?
The diagnosis of MGUS is usually made from blood and urine tests, and in some cases, a bone marrow biopsy. Doctors use specific criteria to distinguish MGUS from related diseases such as smoldering myeloma and multiple myeloma.
MGUS is diagnosed when all of the following are true:
-
A small amount of monoclonal protein (M-protein) is detected in the blood (less than 30 g/L).
-
Fewer than 10% plasma cells are present in the bone marrow.
-
There is no organ damage related to the plasma cells (no bone lesions, anemia, kidney failure, or high calcium).
The M-protein can be detected using specialized laboratory tests, and if the amount increases or other findings develop, further evaluation may be needed to rule out progression.
What additional tests may be performed?
Several tests help confirm the diagnosis of MGUS and provide a baseline for future monitoring.
Serum protein electrophoresis
This test separates proteins in the blood into visible peaks or bands. In MGUS, there is a small, narrow peak representing the abnormal monoclonal protein. The amount of this protein helps distinguish MGUS from more serious plasma cell disorders.
Immunofixation
Immunofixation identifies the type of M-protein made by the plasma cells. Each antibody has two parts: a heavy chain (IgG, IgA, IgM, IgD, or IgE) and a light chain (kappa or lambda). Your report may say, for example, IgG kappa or IgM lambda MGUS. This information helps your doctor determine which tests are needed for follow-up.
Serum free light chain assay
This test measures the amount of free light chains (kappa and lambda) in the blood and calculates their ratio. A small imbalance may occur in MGUS, but the levels are not as abnormal as in multiple myeloma. Tracking these results over time helps detect early changes.
Bone marrow biopsy
Some patients undergo a bone marrow biopsy to confirm that the number of plasma cells is below 10% and that the cells look normal under the microscope. The biopsy may also include immunohistochemistry or flow cytometry to confirm that the plasma cells are monoclonal (producing only kappa or only lambda light chains).
Imaging studies
Because MGUS does not cause bone damage, imaging tests such as X-rays, CT scans, or MRIs are usually normal. These tests may be ordered if a patient has unexplained bone pain to rule out myeloma.
What does monoclonal gammopathy of undetermined significance look like under the microscope?
If a bone marrow biopsy is performed, your pathologist may see a small number of plasma cells scattered among normal bone marrow cells. The plasma cells look similar to normal ones, with round nuclei and abundant blue cytoplasm.
Special tests such as immunohistochemistry or in situ hybridization confirm that all the plasma cells produce one type of light chain (either kappa or lambda), proving that they come from a single abnormal clone. However, there is no evidence of invasive growth or tissue damage, which distinguishes MGUS from myeloma.
How is monoclonal gammopathy of undetermined significance different from multiple myeloma?
MGUS and multiple myeloma are part of the same disease spectrum but differ in severity.
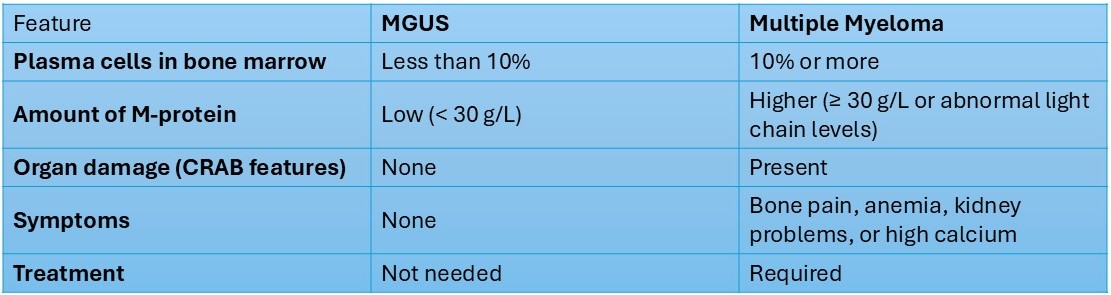
MGUS can remain stable for decades, but a small percentage (about 1% per year) may progress to myeloma or another related condition.
What are the types of monoclonal gammopathy of undetermined significance?
MGUS is classified based on the type of antibody (immunoglobulin) produced by the plasma cells.
Non-IgM MGUS (most common)
Usually involves IgG or IgA antibodies and can occasionally progress to multiple myeloma or light chain amyloidosis.
IgM MGUS
Involves IgM antibodies and may progress to Waldenström macroglobulinemia, a rare lymphoma involving the bone marrow and lymph nodes.
Light chain MGUS
Caused by plasma cells that make only light chains (kappa or lambda) instead of full antibodies. It may progress to multiple myeloma or amyloidosis.
What information will my pathology report include?
Your pathology or laboratory report for MGUS may contain the following details:
-
The type of M-protein (for example, IgG kappa).
-
The amount of M-protein measured in the blood.
-
The kappa/lambda light chain ratio.
-
The percentage of plasma cells in the bone marrow (if a biopsy was done). Plasma cells can be variable in number in the different parts of the biopsy (the aspirate smear and core biopsy material) and your report will be based on the highest percentage of plasma cells seen.
-
A statement confirming the absence of organ damage (CRAB features).
These findings help your doctor confirm that your condition meets the criteria for MGUS and not a more advanced disorder.
What is the prognosis for monoclonal gammopathy of undetermined significance?
The outlook for MGUS is excellent. Most people never develop symptoms or progress to cancer. However, because a small number of patients do develop myeloma or related diseases, regular follow-up is important.
Your doctor will usually recommend:
-
Blood tests every 6 to 12 months to check M-protein levels.
-
Monitoring for new symptoms, such as bone pain, fatigue, or changes in kidney function.
If the M-protein increases significantly or symptoms appear, your doctor may order new tests to look for progression.
Questions to ask your doctor
-
What type of MGUS do I have (IgG, IgA, IgM, or light chain)?
-
What is the level of M-protein in my blood?
-
Do I need a bone marrow biopsy or imaging tests?
-
How often should I have follow-up blood tests?
-
What symptoms should I watch for that might suggest progression?
-
What is my risk of developing multiple myeloma or another condition?
We are proud to partner with:
![]()