
by Jason Wasserman MD PhD FRCPC
September 8, 2022
What is non-intestinal-type sinonasal adenocarcinoma?
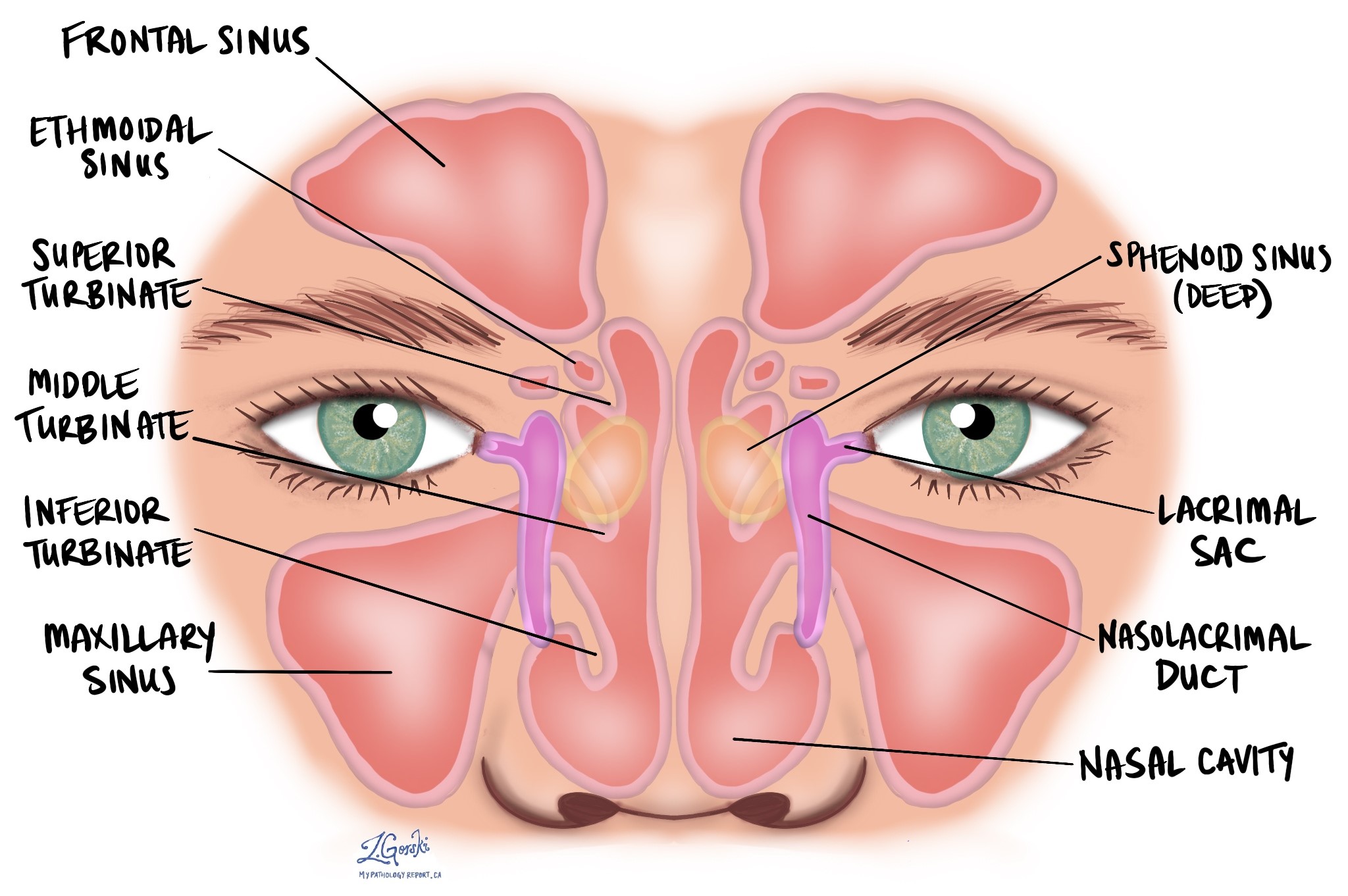
Non-intestinal-type sinonasal adenocarcinoma (SNAC) is a rare type of head and neck cancer. The tumour starts from the tissue that lines the inside of the nasal cavity or the paranasal sinuses such as the ethmoid or maxillary sinus. Pathologists divide non-intestinal-type SNAC into two grades, low and high, with high-grade tumours being associated with more aggressive behaviour and worse overall outcome.
What causes non-intestinal-type sinonasal adenocarcinoma?
At present, doctors do not know what causes non-intestinal-type SNAC. Rare tumours have been associated with human papillomavirus (HPV) but this virus is not believed to cause most non-intestinal-type SNACs.
How is the diagnosis of non-intestinal-type adenocarcinoma made?
The diagnosis of non-intestinal-type SNAC is usually made after a small sample of tissue is removed in a procedure called a biopsy. The diagnosis can also be made after the entire tumour is removed in a procedure called a resection. The tissue is then sent to a pathologist who examines it under a microscope.
What does grade mean and why is it important for non-intestinal-type sinonasal adenocarcinoma?
Pathologists divide non-intestinal-type SNAC into two grades, high and low, based on the way the tumour cells look when examined under the microscope. The grade is important because low-grade tumours may grow into surrounding tissues but are more likely to be cured by surgery alone. In contrast, high-grade tumours grow more quickly and are more likely to spread to other parts of the body such as lymph nodes in the neck.
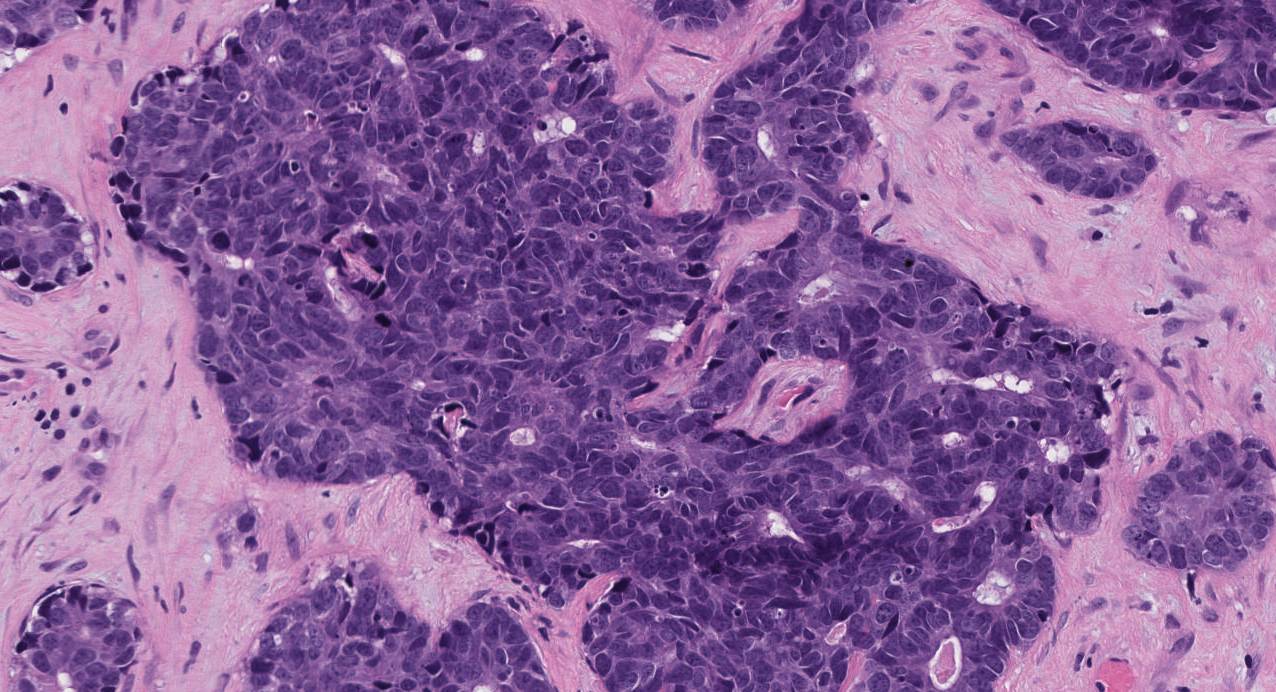
Low-grade non-intestinal-type sinonasal adenocarcinoma
Low-grade tumours are made up of medium-sized cells that contain a specialized type of protein called mucin. The tumour cells often connect together to form round structures called glands or long finger-like projections called papillae. The glands may be arranged in a back-to-back manner that pathologists describe as cribriform. Dividing cells called mitotic figures and a type of cell death called necrosis are rarely seen in low-grade non-intestinal-type SNAC.
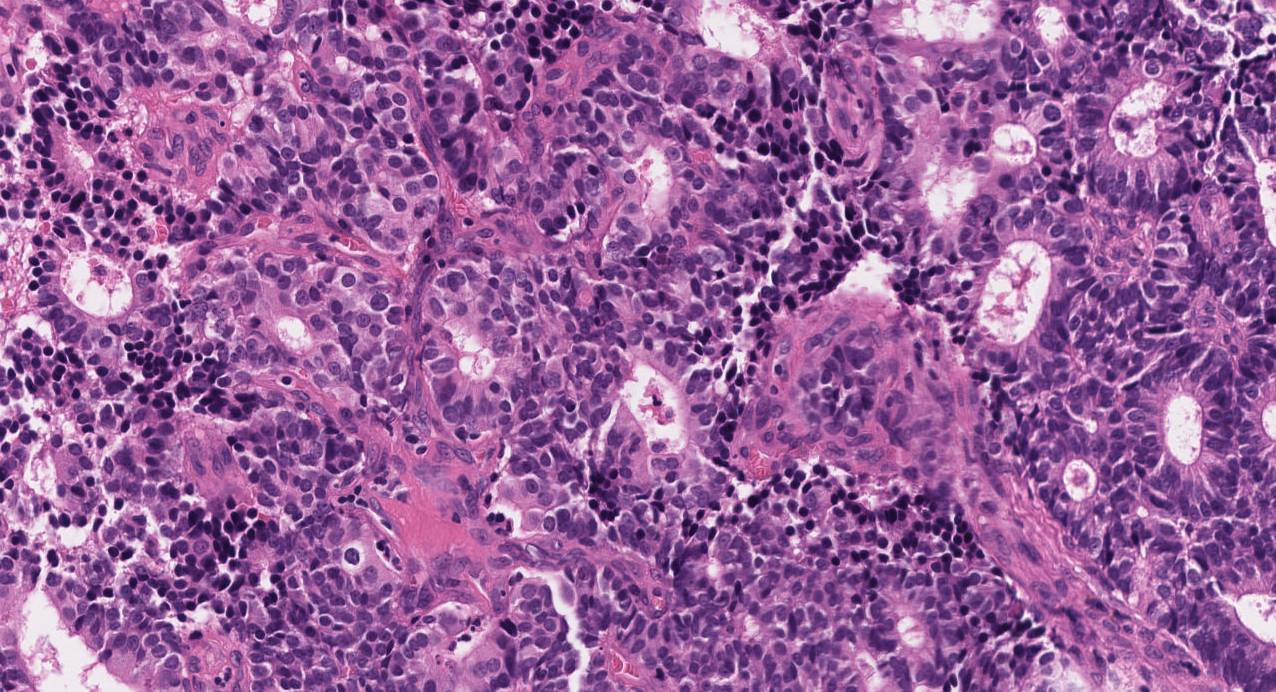
High-grade non-intestinal-type sinonasal adenocarcinoma
High-grade tumours are often made up of larger more abnormal-looking cells that contain less mucin than low-grade tumours. Pathologists use the word atypical to describe abnormal-looking cells. The tumour cells are often connected together into large groups that pathologists describe as a solid pattern of growth. Unlike low-grade tumours, dividing tumour cells called mitotic figures and a type of cell death called necrosis are commonly seen.
What other tests are performed to confirm the diagnosis of non-intestinal-type sinonasal adenocarcinoma?
Your pathologists may perform a test called immunohistochemistry to confirm the diagnosis. When performed, the tumour cells in non-intestinal-type SNAC are usually positive for specialized proteins called cytokeratins including CK7. Very rarely the tumour cells may be positive for proteins normally seen in the gastrointestinal tract such as CK20. High-grade non-intestinal-type SNACs may produce proteins made by neuroendocrine cells such as chromogranin and synaptophysin.
Can non-intestinal-type sinonasal adenocarcinoma spread to other parts of the body?
Low-grade non-intestinal-type SNACs very rarely metastasizes (spreads) to lymph nodes or other parts of the body and are cured by surgery alone. High-grade non-intestinal-type SNACs are more likely to metastasize to other parts of the body, however, the overall risk is still low.
What is lymphovascular invasion and why is it important?
Lymphovascular invasion means that cancer cells were seen inside a blood vessel or lymphatic vessel. Blood vessels are long thin tubes that carry blood around the body. Lymphatic vessels are similar to small blood vessels except that they carry a fluid called lymph instead of blood. The lymphatic vessels connect with small immune organs called lymph nodes that are found throughout the body. Lymphovascular invasion is important because cancer cells can use blood vessels or lymphatic vessels to spread to other parts of the body such as lymph nodes or the lungs. If lymphovascular invasion is seen, it will be included in your report.

What is perineural invasion and why is it important?
Perineural invasion is a term pathologists use to describe cancer cells attached to or inside a nerve. A similar term, intraneural invasion, is used to describe cancer cells inside a nerve. Nerves are like long wires made up of groups of cells called neurons. Nerves are found all over the body and they are responsible for sending information (such as temperature, pressure, and pain) between your body and your brain. Perineural invasion is important because the cancer cells can use the nerve to spread into surrounding organs and tissues. This increases the risk that the tumour will regrow after surgery. If perineural invasion is seen, it will be included in your report.

Were lymph nodes examined and did any contain cancer cells?
Lymph nodes are small immune organs found throughout the body. Cancer cells can spread from a tumour to lymph nodes through small vessels called lymphatics. Lymph nodes are not always removed at the same time as the tumour. However, when lymph nodes are removed, they will be examined under a microscope and the results will be described in your report.

Cancer cells typically spread first to lymph nodes close to the tumour although lymph nodes far away from the tumour can also be involved. For this reason, the first lymph nodes removed are usually close to the tumour. Lymph nodes further away from the tumour are only typically removed if they are enlarged and there is a high clinical suspicion that there may be cancer cells in the lymph node. Most reports will include the total number of lymph nodes examined, where in the body the lymph nodes were found, and the number (if any) that contain cancer cells. If cancer cells were seen in a lymph node, the size of the largest group of cancer cells (often described as “focus” or “deposit”) will also be included.
The examination of lymph nodes is important for two reasons. First, this information is used to determine the pathologic nodal stage (pN). Second, finding cancer cells in a lymph node increases the risk that cancer cells will be found in other parts of the body in the future. As a result, your doctor will use this information when deciding if additional treatment such as chemotherapy, radiation therapy, or immunotherapy is required.
What does it mean if a lymph node is described as positive?
Pathologists often use the term “positive” to describe a lymph node that contains cancer cells. For example, a lymph node that contains cancer cells may be called “positive for malignancy” or “positive for metastatic carcinoma”.
What does it mean if a lymph node is described as negative?
Pathologists often use the term “negative” to describe a lymph node that does not contain any cancer cells. For example, a lymph node that does not contain cancer cells may be called “negative for malignancy” or “negative for metastatic carcinoma”.
What does extranodal extension mean?
All lymph nodes are surrounded by a thin layer of tissue called a capsule. Extranodal extension means that cancer cells within the lymph node have broken through the capsule and have spread into the tissue outside of the lymph node. Extranodal extension is important because it increases the risk that the tumour will regrow in the same location after surgery. For some types of cancer, extranodal extension is also a reason to consider additional treatment such as chemotherapy or radiation therapy.
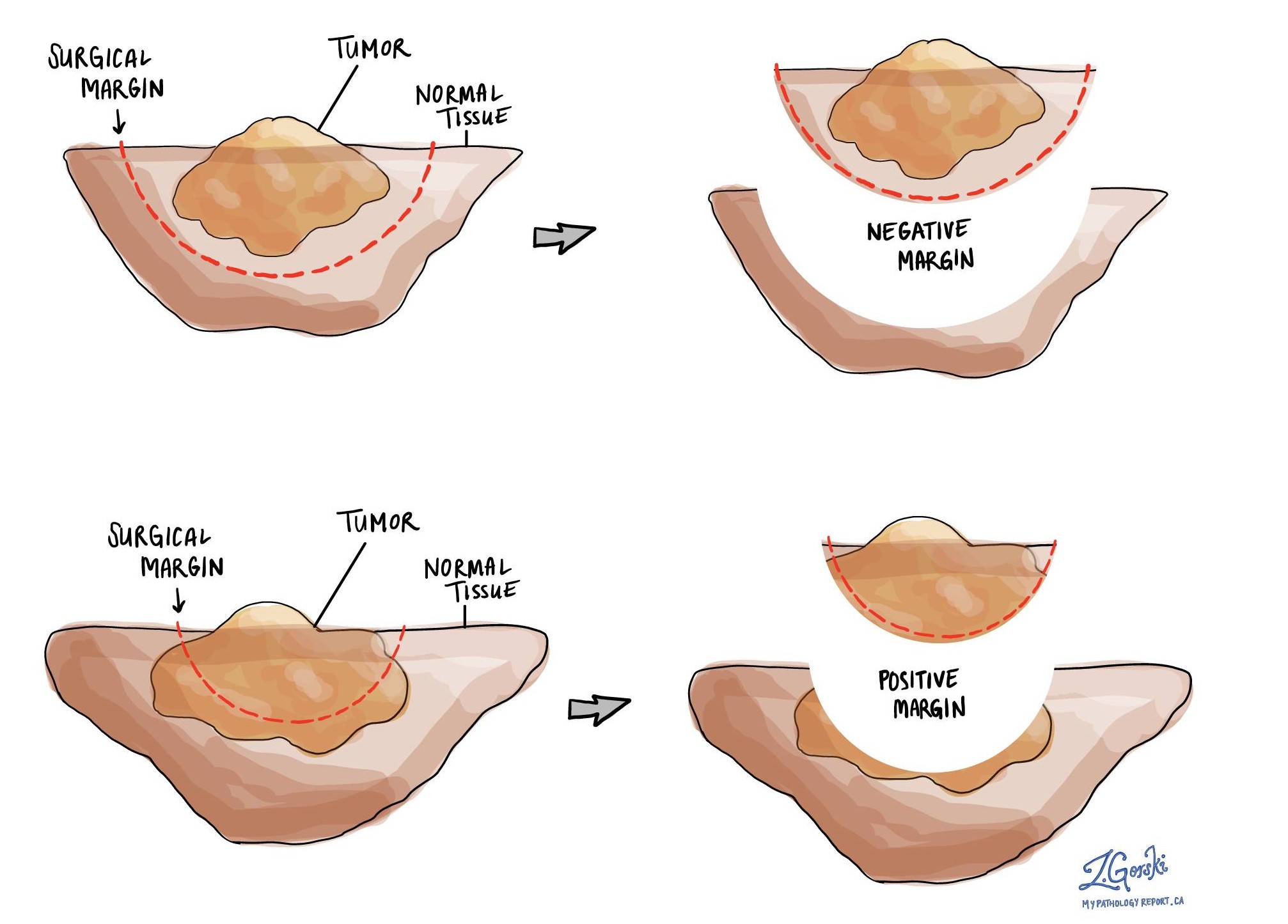
What is a margin?
In pathology, a margin is the edge of a tissue that is cut when removing a tumour from the body. The margins described in a pathology report are very important because they tell you if the entire tumour was removed or if some of the tumour was left behind. The margin status will determine what (if any) additional treatment you may require.
Most pathology reports only describe margins after a surgical procedure called an excision or resection has been performed for the purpose of removing the entire tumour. For this reason, margins are not usually described after a procedure called a biopsy is performed for the purpose of removing only part of the tumour. Because non-intestinal-type SNAC is often removed in multiple pieces, your pathologist may not be able to determine the margin status.
Pathologists carefully examine the margins to look for tumour cells at the cut edge of the tissue. If tumour cells are seen at the cut edge of the tissue, the margin will be described as positive. If no tumour cells are seen at the cut edge of the tissue, a margin will be described as negative. Even if all of the margins are negative, some pathology reports will also provide a measurement of the closest tumour cells to the cut edge of the tissue.
A positive (or very close) margin is important because it means that tumour cells may have been left behind in your body when the tumour was surgically removed. For this reason, patients who have a positive margin may be offered another surgery to remove the rest of the tumour or radiation therapy to the area of the body with the positive margin. The decision to offer additional treatment and the type of treatment options offered will depend on a variety of factors including the type of tumour removed and the area of the body involved.
How do pathologists determine the pathologic stage (pTNM) for non-intestinal-type sinonasal adenocarcinoma?
The pathologic stage for non-intestinal-type SNAC is based on the TNM staging system, an internationally recognized system originally created by the American Joint Committee on Cancer. This system uses information about the primary tumour (pT), lymph nodes (pN), and distant metastatic disease (pM) to determine the complete pathologic stage (pTNM). Your pathologist will examine the tissue submitted and give each part a number. In general, a higher number means more advanced disease and a worse prognosis.
Tumour stage (pT) for tumours that start in the nasal cavity or ethmoid sinus
These tumours are given a tumour stage between 1 and 4. The tumour stage is based on how far the tumour has spread outside of the nasal cavity or ethmoid sinus.
- T1 – The tumour is limited to the nasal cavity or ethmoid sinus. It has not extended into the surrounding bones.
- T2 – The tumour has spread out of the nasal cavity or ethmoid sinus.
- T3 – The tumour has spread into the wall or floor of the orbit (the cavity that holds the eye), maxillary sinus, palate (the roof of the mouth), or cribriform plate (an area at the top of the nasal cavity).
- T4 – The tumour has spread to the eye, skin of the nose or cheek, cranial cavity (the space that holds the brain), pterygoid plates (bones at the bottom of the cranial cavity), sphenoid or frontal sinuses.
Tumour stage (pT) for tumours that start in the maxillary sinus
These tumours are given a tumour stage between 1 and 4. The tumour stage is based on how far the tumour has spread outside of the maxillary sinus.
- T1 – The tumour is limited to the maxillary sinus. It has not extended into the surrounding bones.
- T2 – The tumour has spread out of the nasal cavity or ethmoid sinus.
- T3 – The tumour has spread into the bone at the back of the maxillary sinus, subcutaneous tissues, floor or wall of the orbit (the cavity that holds the eye), pterygoid fossa, or ethmoid sinuses.
- T4 – The tumour has spread to the eye, skin of the nose or cheek, cranial cavity (the space that holds the brain), pterygoid plates (bones at the bottom of the cranial cavity), sphenoid or frontal sinuses.
Nodal stage (pN) for tumours that start in the nasal cavity or paranasal sinuses
These tumours are given a nodal stage between 0 and 3 based on the following three features:
- The number of lymph nodes that contain cancer cells.
- The size of the tumour deposit.
- Whether the lymph nodes with cancer cells are on the same side (ipsilateral) or the opposite side (contralateral) of the tumour.
The nodal stage will be higher if any of the tumour deposits are larger than 3 cm, more than one lymph node contains cancer cells, cancer cells are found in lymph nodes on both sides of the neck, and if any of the lymph nodes show extranodal extension.
If no cancer cells are found in any of the lymph nodes examined, the nodal stage is N0. If no lymph nodes are submitted for pathological examination, the nodal cannot be determined and the stage is listed as NX.
Metastatic stage (pM) for non-intestinal type sinonasal adenocarcinoma
Non-intestinal-type SNAC is given a metastatic stage (pM) of 0 or 1 based on the presence of cancer cells at a distant site in the body (for example the lungs). The metastatic stage can only be determined if tissue from a distant site is submitted for pathological examination. Because this tissue is rarely present, the metastasis stage cannot be determined and is listed as MX.
We are proud to partner with:
![]()
Our work is generously supported by:
![]()