

In pathology, the word amorphous means “without a clear shape or structure.” When a pathologist uses this term in a report, it describes material seen under the microscope that appears shapeless, featureless, or disorganized — lacking the defined outlines and patterns of normal cells or tissue. Amorphous material is not a diagnosis on its own, but it is an important clue that something unusual is present in the tissue. Depending on what else is found in the sample, it can help identify specific diseases or explain changes caused by cell breakdown, protein deposits, or mineral buildup.
When do pathologists see amorphous material?
Amorphous material can appear in tissue samples for several different reasons:
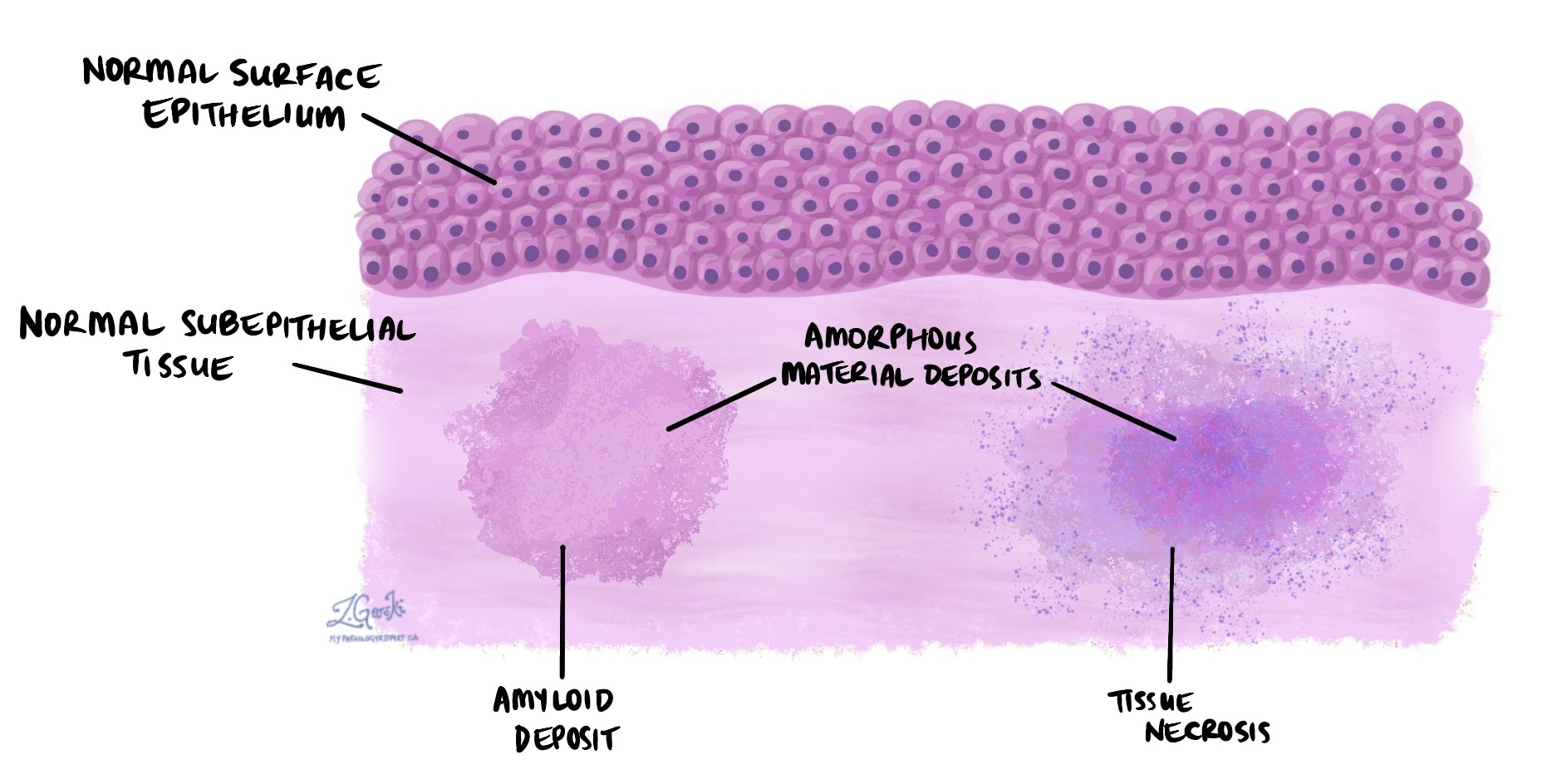
- Necrosis — when cells die, they break down and lose their normal shape. The resulting debris often appears amorphous under the microscope. This can occur in rapidly growing cancers, areas of poor blood supply, or severe infections.
- Amyloid deposits — amyloid is an abnormal protein that can accumulate in tissues in conditions collectively known as amyloidosis. Under the microscope, amyloid appears as pale pink, structureless (amorphous) deposits that have no recognizable cell pattern.
- Calcifications — calcium deposits within tissue can appear as irregular, amorphous material, particularly when they form in areas of prior cell death or chronic inflammation.
- Tumors — some cancers and benign tumors contain amorphous material in the background of the tissue, produced by the breakdown of tumor cells or by the secretion of unusual substances such as mucin or keratin.
- Inflammation — in areas of active or chronic inflammation, proteins leak out of damaged blood vessels and cells break down, creating amorphous deposits in the surrounding tissue.
How do pathologists identify what amorphous material is made of?
Because amorphous material has no recognizable structure, standard microscopic examination alone often cannot determine what it is. Pathologists use special stains and additional tests to identify the substance:
- Congo red stain — used specifically to detect amyloid. Amyloid turns pink under regular light and exhibits a characteristic apple-green glow under polarized light, confirming the diagnosis of amyloidosis.
- PAS (Periodic acid-Schiff) stain — highlights carbohydrates and certain proteins, including mucin. Useful for identifying glycogen deposits, fungal organisms, or mucin-producing cells within amorphous areas.
- Calcium stains — stains such as von Kossa highlight mineral deposits in tissue, confirming that amorphous material contains calcium.
- Immunohistochemistry (IHC) — uses antibodies to detect specific proteins within amorphous material, helping to determine whether it contains tumor markers, immune proteins, or other identifiable substances.
What does amorphous material in my report mean?
Seeing the word “amorphous” in a pathology report means the pathologist observed structureless material that required description and further analysis. By itself, it is a descriptive term — not a diagnosis. The significance of amorphous material depends entirely on its context: where it was found, how much is present, what it is made of, and what other findings appear alongside it in the report.
In many cases, the pathologist will have already identified what the amorphous material represents and will state this elsewhere in the report — for example, “amorphous deposits consistent with amyloid” or “amorphous necrotic debris.” If you are uncertain what the amorphous material in your report refers to, your doctor can explain the finding in the context of your full diagnosis.
Questions to ask your doctor
- What is the amorphous material in my report made of, and what does it represent?
- Is this finding related to my main diagnosis, or is it an incidental observation?
- Does it require any further testing or affect my treatment plan?
Related articles on MyPathologyReport.com
We are proud to partner with:
![]()