

Reviewed by Pathologists on:
January 13, 2026
The Banff score is a standardized system used to describe findings in a kidney transplant biopsy. It is part of the Banff Classification, an international consensus system that enables transplant teams worldwide to interpret biopsy results in a consistent and meaningful way.
The Banff score is not a single number. Instead, it is made up of multiple individual elements, each describing a specific type of change in a particular part of the kidney. These elements are then combined using established rules to determine whether rejection or another form of injury is present and, if so, how severe it is.
What does rejection mean?
Rejection occurs when the recipient’s immune system recognizes the transplanted kidney as foreign and mounts an attack against it. This attack can happen in two main ways.
Immune cell–mediated rejection occurs when immune cells, especially T cells, migrate into kidney tissue and directly damage it. These cells can infiltrate the spaces between tubules, invade the tubules themselves, or damage arteries.
- The Banff elements i, t, v, ti, i-IFTA, and t-IFTA are especially important for identifying this type of rejection.
Antibody-mediated rejection occurs when the immune system produces antibodies that bind to the blood vessels of the transplanted kidney. This leads to injury of small blood vessels and impaired blood flow.
- The Banff elements g, ptc, C4d, cg, and ptcml help identify this type of rejection.
Understanding how the immune system injures the kidney is critical because treatments differ depending on the mechanism.
Anatomy of the kidney
To understand the Banff score, it helps to know the basic microscopic parts of the kidney and what they normally do. A kidney biopsy looks at these structures in great detail under the microscope.
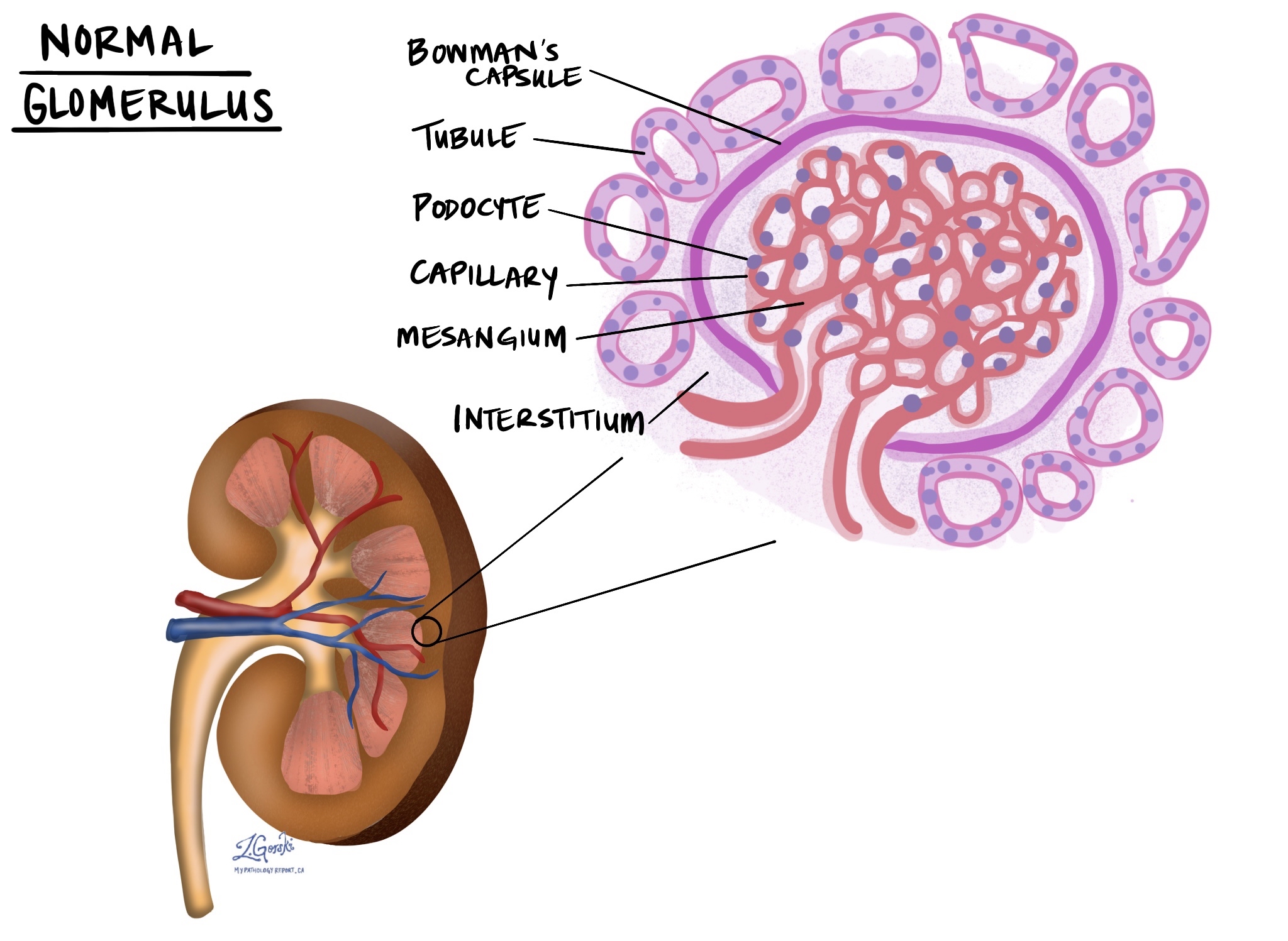
- Glomerulus: The glomerulus is a tiny ball-shaped structure that acts as a filter. Its job is to remove waste products and excess fluid from the bloodstream while keeping important proteins and cells inside. Each kidney contains millions of glomeruli.
- Bowman’s capsule: Bowman’s capsule is a thin, cup-like structure that surrounds the glomerulus. It collects the filtered fluid from the glomerulus and directs it into the tubules. Damage here can interfere with the first step of urine formation.
- Podocytes: Podocytes are specialized cells that wrap around the outside of the glomerular capillaries. They form part of the filtration barrier and help prevent proteins from leaking into the urine. Injury to podocytes can lead to protein loss and kidney dysfunction.
- Mesangium: The mesangium is a supportive tissue located in the center of the glomerulus. It helps hold the glomerular capillaries in place and regulates blood flow within the filter. Inflammation or expansion of the mesangium can affect how well the glomerulus works.
- Capillaries: Capillaries are very small blood vessels. In the kidney, they are found inside the glomerulus and around the tubules. These vessels deliver blood for filtration and supply oxygen and nutrients. Many Banff scores assess inflammation or injury in these tiny vessels.
- Tubules: Tubules are long, narrow channels that process the fluid filtered by the glomerulus. As fluid moves through the tubules, useful substances such as water, salts, and nutrients are reabsorbed, and waste products are concentrated into urine. Damage to tubules can impair urine formation and kidney function.
- Interstitium: The interstitium is the supportive tissue located between tubules, blood vessels, and other kidney structures. Normally, it contains very few immune cells. Inflammation or scarring in the interstitium is a key feature assessed by several Banff scores.
How kidney structures relate to Banff scores
Each Banff score corresponds to immune injury in a specific part of the kidney. Inflammation in the interstitium is measured by the i and ti scores, while immune cells invading the tubules are captured by the t and t-IFTA scores. Injury to the glomerulus, the kidney’s filtering unit, is assessed by the g score, while chronic damage to the glomerular filtration barrier is reflected by the cg score. Inflammation in the tiny blood vessels around tubules, called peritubular capillaries, is measured by the ptc and pvl scores, and long-term damage to these vessels is reflected by ptcml. Immune injury to arteries is captured by the v score, while chronic scarring of kidney tissue and blood vessels is described by ci, ct, and cv. Together, these scores map where immune injury is occurring, whether it is active or long-standing, and whether it is driven mainly by immune cells or antibodies.
Banff elements explained
i – Interstitial inflammation (score 0–3)
The interstitium is the supportive tissue that lies between kidney tubules. Under normal conditions, it contains very few immune cells. The i score measures how much of this tissue is affected by inflammation.
-
i0: No or minimal inflammation.
-
i1: Inflammation affecting 10–25% of the kidney tissue.
-
i2: Inflammation affecting 26–50% of the tissue.
-
i3: Inflammation affecting more than 50% of the tissue.
Higher scores indicate more widespread immune activity and greater concern for rejection.
t – Tubulitis (score 0–3)
Tubules are small, tube-like structures that process filtered blood to form urine. They are essential for removing waste and balancing fluids and electrolytes. The t score measures the number of immune cells that have entered the tubular lining.
-
t0: No immune cells in the tubules.
-
t1: A small number of immune cells in the tubules.
-
t2: A moderate number of immune cells.
-
t3: A large number of immune cells or evidence of tubule damage.
Tubulitis is a key feature of active immune attack on the kidney.
v – Intimal arteritis (score 0–3)
Arteries supply oxygen-rich blood to the kidneys. Damage to the arteries can severely impair kidney function. The v score measures inflammation within the inner layer of arteries.
-
v0: No artery inflammation.
-
v1: Mild inflammation affecting part of the artery lining.
-
v2: More severe inflammation causing narrowing of the artery.
-
v3: Severe inflammation with extensive arterial wall damage.
Arterial involvement usually indicates more severe rejection.
g – Glomerulitis (score 0–3)
Glomeruli are tiny filters that remove waste from the blood. The g score measures inflammation within these filtering units.
-
g0: No inflammation in glomeruli.
-
g1: Inflammation in a small proportion of glomeruli.
-
g2: Inflammation in a moderate proportion.
-
g3: Inflammation in most glomeruli.
Glomerulitis is commonly associated with antibody-mediated rejection.
ptc – Peritubular capillaritis (score 0–3)
Peritubular capillaries are small blood vessels surrounding the tubules that supply oxygen and nutrients. The ptc score measures immune cells inside these capillaries.
-
ptc0: No capillary inflammation.
-
ptc1: Mild capillary inflammation.
-
ptc2: Moderate capillary inflammation.
-
ptc3: Severe capillary inflammation.
Together with glomerulitis, a higher ptc score reflects microvascular injury.
C4d – Complement deposition (score 0–3)
C4d is a protein produced when antibodies activate the immune system along blood vessel walls. The C4d score measures how much of the capillary network shows this protein.
-
C4d0: No staining.
-
C4d1: Minimal staining.
-
C4d2: Moderate staining.
-
C4d3: Extensive staining.
Positive C4d supports a diagnosis of antibody-mediated rejection when interpreted alongside other findings.
ci – Interstitial fibrosis (score 0–3)
Fibrosis means scarring of kidney tissue. The ci score measures how much of the interstitial tissue has been replaced by scar.
-
ci0: No scarring.
-
ci1: Mild scarring.
-
ci2: Moderate scarring.
-
ci3: Severe scarring.
A higher ci score reflects chronic, long-standing injury.
ct – Tubular atrophy (score 0–3)
Tubular atrophy means tubules have shrunk or lost function. The ct score measures how many tubules are affected.
-
ct0: No atrophy.
-
ct1: Mild atrophy.
-
ct2: Moderate atrophy.
-
ct3: Severe atrophy.
This also represents chronic damage.
cv – Vascular fibrous intimal thickening (score 0–3)
The cv score measures scarring inside arteries that narrows blood flow to the kidneys.
-
cv0: No arterial thickening.
-
cv1: Mild narrowing.
-
cv2: Moderate narrowing.
-
cv3: Severe narrowing.
A higher cv score indicates long-term vascular injury.
cg – Glomerular basement membrane double contours (score 0–3)
The basement membrane supports glomerular filters. The cg score measures thickening and duplication of this membrane.
-
cg0: Normal basement membrane.
-
cg1: Mild duplication.
-
cg2: Moderate duplication.
-
cg3: Severe duplication.
This finding defines transplant glomerulopathy, a chronic antibody-mediated injury.
ptcml – Peritubular capillary basement membrane multilayering (present/absent)
The ptcml score describes thickening of capillary walls seen with specialized testing. When present, it supports chronic antibody-mediated rejection.
ti – Total inflammation (score 0–3)
The ti score measures inflammation throughout the kidney cortex, including in scarred areas.
-
ti0: Minimal inflammation.
-
ti1: Mild inflammation.
-
ti2: Moderate inflammation.
-
ti3: Severe inflammation.
The ti score reflects the overall immune burden with a higher score indicating more inflammation throughout the kidney.
i-IFTA – Inflammation in scarred areas (score 0–3)
The i-IFTA score measures immune cells within already scarred tissue.
-
i-IFTA0: No inflammation in scarred areas.
-
i-IFTA1: Mild inflammation.
-
i-IFTA2: Moderate inflammation.
-
i-IFTA3: Severe inflammation.
A higher i-IFTA score indicates chronic active rejection.
t-IFTA – Tubulitis in scarred areas (score 0–3)
The t-IFTA score measures immune cells invading tubules located in scarred tissue.
-
t-IFTA0: No tubulitis.
-
t-IFTA1: Mild tubulitis.
-
t-IFTA2: Moderate tubulitis.
-
t-IFTA3: Severe tubulitis.
The t-IFTA score also indicates ongoing immune injury.
pvl – Peritubular capillary inflammation with lymphocytes (present/absent)
The pvl score describes lymphocyte-predominant inflammation in small capillaries and provides additional detail about immune activity.
How do these scores lead to severity grades?
Banff scores are combined to assign a diagnostic category and severity grade.
For T cell–mediated rejection:
-
Borderline: Mild changes that may not require treatment.
-
Type IA: Interstitial inflammation and tubulitis without artery involvement.
-
Type IB: More severe tubulitis.
-
Type II–III: Arterial involvement, indicating severe rejection.
Higher grades mean stronger immune attack and usually require more aggressive treatment.
Questions to ask your doctor
-
Which Banff elements were abnormal in my biopsy?
-
Do these findings suggest immune cell– or antibody-mediated rejection?
-
What severity grade applies to my case?
-
Are the changes active, chronic, or both?
-
How will this affect my treatment and follow-up?
We are proud to partner with:
![]()