

by Jason Wasserman MD PhD FRCPC
March 11, 2026
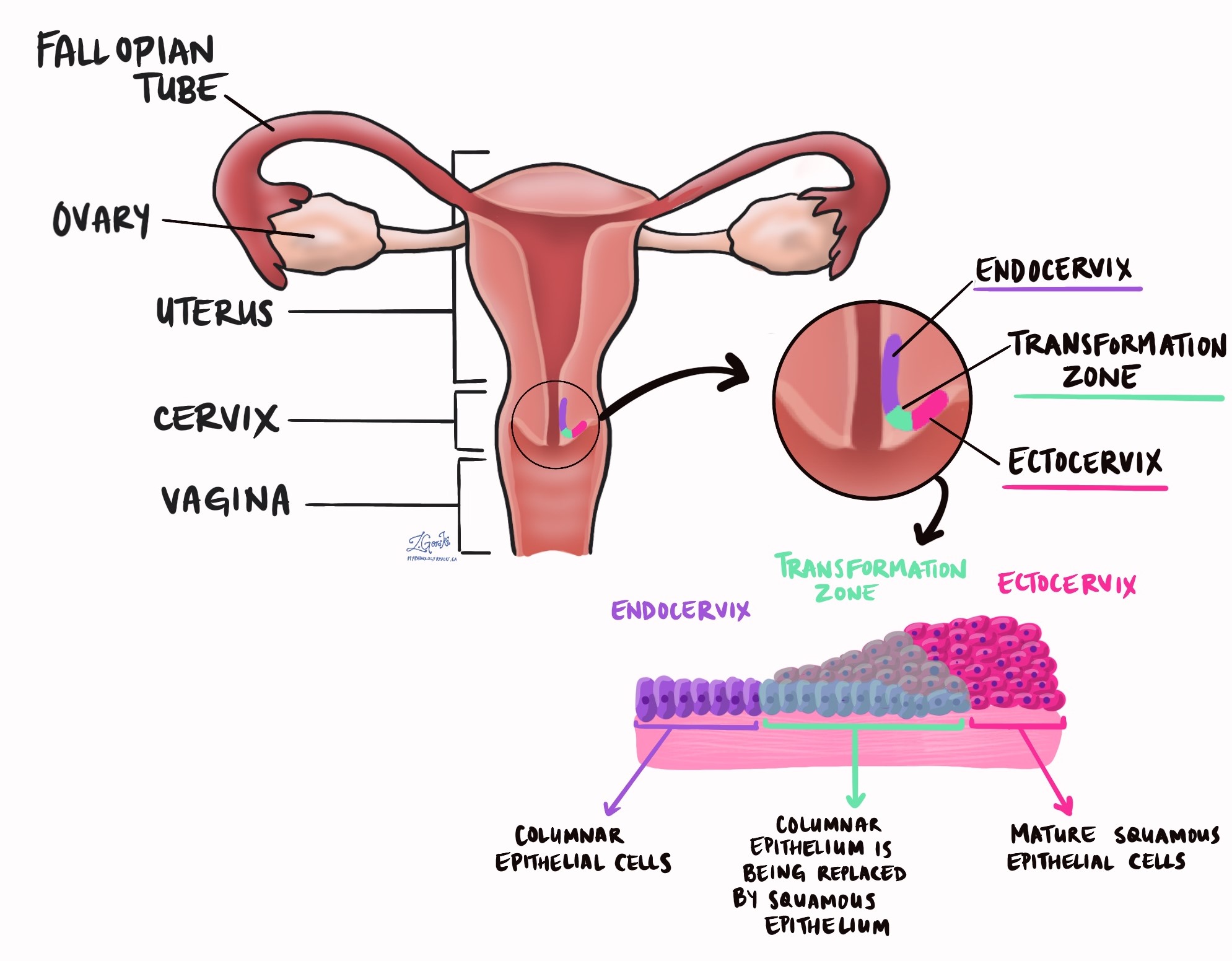
HPV-associated adenocarcinoma is a type of cervical cancer that develops from glandular cells in the cervix. Glandular cells produce mucus and line the cervical canal, which connects the uterus to the vagina.
This cancer is called HPV-associated because it is caused by infection with high-risk types of human papillomavirus (HPV). Persistent infection with these viruses can damage the DNA of cervical cells, allowing them to grow uncontrolled.
HPV-associated adenocarcinoma most often develops in the transformation zone, the area where glandular cells inside the cervix meet squamous cells on the outer surface. Compared with HPV-independent cervical adenocarcinomas, HPV-associated tumors usually occur at a younger age and generally have a better prognosis.
What are the symptoms of HPV-associated adenocarcinoma of the cervix?
The symptoms of HPV associated adenocarcinoma of the cervix vary. Some patients develop symptoms related to the tumor, while others are diagnosed through cervical cancer screening.
The most common symptom is abnormal vaginal bleeding, such as bleeding after sexual intercourse, between menstrual periods, or after menopause. Some patients may notice abnormal vaginal discharge or pelvic pain.
Because cervical screening can detect abnormal glandular cells, some cases are discovered before symptoms develop.
What causes HPV-associated adenocarcinoma?
HPV-associated adenocarcinoma develops after long-term infection with high-risk types of HPV, most commonly HPV types 18, 16, and 45.
HPV infection is very common and is usually cleared by the immune system. In some people, the infection persists. Viral proteins produced by HPV interfere with normal cell-cycle control by inactivating key proteins that normally regulate cell growth. Over time, these changes can lead to abnormal cell growth and eventually cancer.
Additional genetic changes may occur as the tumor develops, including mutations in genes involved in cell growth pathways.
How is this diagnosis made?
The diagnosis of HPV-associated adenocarcinoma usually begins with cervical screening tests.
Abnormal results on a Pap test or HPV test may lead to further evaluation with colposcopy. This procedure allows the cervix to be examined closely and small tissue samples to be taken.
The diagnosis is confirmed when a pathologist examines cervical tissue under the microscope. The tissue may be obtained through a biopsy, endocervical curettage, or a procedure such as a cone biopsy or loop electrosurgical excision procedure (LEEP).
If surgery is performed, the pathologist also examines the removed tissue to determine the size of the tumor, how deeply it has grown into the cervix, and whether it has spread to nearby structures.
Microscopic features
Under the microscope, HPV-associated adenocarcinoma forms irregular glands that invade the supporting tissue of the cervix.
The tumor cells typically have enlarged, elongated nuclei that appear darker than normal and may contain visible nucleoli. The glands are often lined by tall columnar cells that produce mucus.
A characteristic feature of HPV-associated adenocarcinoma is the presence of mitotic figures and apoptotic cells near the surface of the glands, which can often be recognized at low magnification.
Some tumors grow in a destructive, invasive pattern, with irregular glands and clusters of cells infiltrating the cervical tissue and producing a fibrous reaction called desmoplasia. Other tumors show a non-destructive pattern, where the glands remain well-formed and resemble adenocarcinoma in situ.
These patterns can help predict the risk of lymph node spread and recurrence.
Immunohistochemistry
Immunohistochemistry is a laboratory test that uses antibodies to detect specific proteins inside tumor cells. These tests help confirm the diagnosis and demonstrate that HPV infection is driving the cancer.
HPV-associated adenocarcinomas typically show strong, diffuse p16 staining, a protein overexpressed when HPV disrupts normal cell-cycle control.
Other commonly positive markers include CK7 and PAX8, which support a cervical origin of the tumor. Most tumors show wild-type p53 staining and are negative for estrogen receptor (ER), progesterone receptor (PR), and vimentin.
In situ hybridization
In situ hybridization (ISH) is a laboratory test that detects HPV DNA or RNA directly within tumor cells.
This test uses specially designed probes that bind to HPV genetic material within the cells. When HPV is present, the probes produce a visible signal under the microscope.
ISH helps confirm that the tumor is caused by high-risk HPV infection. Tests that detect HPV RNA are generally more specific than tests that detect HPV DNA.
Biomarkers
Biomarker testing examines proteins or other molecular features in tumor cells to help guide treatment decisions. These tests are usually performed on tumor tissue using immunohistochemistry or other laboratory methods. Not all biomarkers are tested in every case, but the results can provide important information about treatment options.
PD-L1
PD-L1 is a protein that helps cancer cells evade immune system detection.
Testing for PD-L1 is performed using immunohistochemistry and is often reported using a combined positive score (CPS). This score measures PD-L1 expression in tumor cells and nearby immune cells.
Tumors that express PD-L1 may respond to immune checkpoint inhibitor therapy, which is sometimes used to treat advanced or recurrent cervical cancer.
Other features to look for in your pathology report
Tumor size and depth of invasion
Once the diagnosis is made, the pathologist measures the tumor to determine its size and how deeply it has grown into the cervix.
Tumor size describes how far the cancer extends along the cervix. Depth of invasion describes how far the tumor has grown from the surface into the supporting tissue of the cervix.
These measurements are important because tumors that invade more deeply are more likely to spread to lymph nodes or nearby organs.
Silva classification
HPV-associated adenocarcinoma of the cervix can grow into the surrounding tissue in different ways. Pathologists sometimes describe these growth patterns using a system called the Silva classification. This system helps estimate how likely the cancer is to spread to lymph nodes or come back after treatment.
The Silva classification divides tumors into three patterns based on how the cancer grows into the cervical tissue.
Pattern A
In this pattern, the cancer forms well-defined glands that remain closely grouped. The glands grow into the cervical tissue but do not show destructive invasion. Cancer cells are not seen in blood vessels or lymphatic vessels. Tumors with Pattern A growth have a very low risk of spreading to lymph nodes or recurring after treatment.
Pattern B
In this pattern, small groups of cancer cells begin to break away from the main glands and invade the surrounding tissue in limited areas. Some tumors with this pattern may show lymphovascular invasion, which means cancer cells are present in small blood vessels or lymphatic channels.
Pattern C
In this pattern, the cancer shows diffuse, destructive invasion into the surrounding tissue. The glands are often irregular and distorted, and the nearby tissue frequently shows a fibrous reaction. Tumors with Pattern C growth are more likely to show lymphovascular invasion and spread to lymph nodes.
Overall, tumors with Pattern A growth usually behave more indolently and have a very low risk of recurrence. Tumors with Pattern B or Pattern C growth have a higher risk of spreading and may require more aggressive treatment.

Tumor spread
Pathologists examine the tumor to determine whether it has spread beyond the cervix.
The tumor may extend into nearby structures such as the vagina, uterus, parametrium, pelvic wall, bladder, or rectum. The parametrium is the fibrous tissue that surrounds the cervix.
The presence of tumor cells in these structures increases the cancer stage and may affect treatment decisions.
Lymphovascular invasion
Lymphovascular invasion means tumor cells are present inside small lymphatic channels or blood vessels in the cervix.
These vessels normally carry fluid or blood through the body. When tumor cells enter these channels, they can travel to nearby lymph nodes or other organs. The presence of lymphovascular invasion increases the risk of cancer spread and may influence treatment planning.
Perineural invasion
Perineural invasion means tumor cells are growing along or around nerves in the cervix.
This pattern may increase the risk of the cancer returning in nearby tissues and may influence the choice of additional treatments such as radiation therapy.
Margins
Margins are the edges of the tissue removed during surgery.
A negative margin means that no cancer cells are present at the edge of the tissue, suggesting that the tumor was completely removed. A positive margin means that cancer cells extend to the edge, which increases the risk that some tumor cells remain.
Margins are evaluated in cone biopsies and hysterectomy specimens.
Lymph nodes
Lymph nodes are small immune organs that help filter harmful substances from the body.
The cervix drains into lymph nodes in the pelvis and abdomen. During surgery for cervical cancer, lymph nodes from these areas may be removed and examined under the microscope.
If tumor cells are found in these lymph nodes, the cancer is considered to have spread beyond the cervix, and the stage increases.
When tumor cells are present in lymph nodes, the pathology report may describe the size of the tumor deposits.
- Isolated tumor cells measure 0.2 mm or less.
- Micrometastases measure more than 0.2 mm but 2 mm or less.
- Macrometastases measure more than 2 mm.
The pathology report may also describe the number of lymph nodes examined, the number containing tumor cells, and the location of involved lymph nodes.
How is HPV associated cervical cancer staged?
Staging describes how far the cancer has spread within the cervix and beyond. It is the most important factor for predicting outcome and deciding on treatment. Two systems are commonly used for cervical cancer: TNM and FIGO.
-
The TNM system records tumor size and spread in the cervix (T), whether lymph nodes contain cancer (N), and whether the cancer has spread to distant organs (M).
-
The FIGO system focuses on how far the cancer has spread beyond the cervix into surrounding tissues, lymph nodes, or distant sites. Gynecologic oncologists widely use it to guide treatment planning.
TNM pathologic stage
-
The letter T describes how far the tumor has grown in and around the cervix.
-
T1a means the tumor is only visible under the microscope and measures no more than 5 millimeters in depth and 7 millimeters in width.
-
T1b means that the tumor is visible or measures deeper than five millimeters or wider than seven millimeters.
-
T2a means that the tumor has spread beyond the cervix and uterus but has not entered the parametrium.
-
T2b means that the tumor has grown into the parametrium.
-
T3a means that the tumor involves the lower part of the vagina.
-
T3b means that the tumor reaches the pelvic wall or blocks a ureter, which can harm the kidneys.
-
T4 means that the tumor has grown into the bladder or rectum or has extended beyond the pelvis.
-
-
The letter N describes lymph nodes.
-
NX means that no nodes were removed.
-
N0 means that no cancer was found in the nodes.
-
N0 with isolated tumor cells means that only tiny clusters smaller than zero point two millimeters were present.
-
N1 means that a larger cancer deposit was found in at least one node.
-
-
The letter M describes distant spread to organs such as the lungs or liver.
FIGO stage
-
Stage I means that the cancer is confined to the cervix.
-
Stage IA1 means that the depth of invasion is three millimeters or less.
-
Stage IA2 means the depth of invasion is between 3 and 5 millimeters.
-
Stage IB1 means that the tumor is two centimetres or smaller.
-
Stage IB2 means the tumor is more than 2 centimetres but no more than 4 centimetres.
-
Stage IB3 means that the tumor is larger than four centimetres.
-
-
Stage II means that the cancer has spread beyond the cervix but not to the pelvic wall or the lower third of the vagina.
-
Stage IIA1 means that the tumor involves the upper vagina and measures four centimetres or less.
-
Stage IIA2 means that the tumor in the upper vagina is larger than four centimetres.
-
Stage IIB means that the tumor extends into the parametrium.
-
-
Stage III means more extensive local spread.
-
Stage IIIA means that the cancer involves the lower third of the vagina.
-
Stage IIIB means that the cancer reaches the pelvic wall or blocks a ureter.
-
Stage IIIC1 means that cancer is present in pelvic lymph nodes.
-
Stage IIIC2 means that cancer is present in para-aortic lymph nodes.
-
-
Stage IV means spread to nearby organs or to distant sites.
-
Stage IVA means invasion of the bladder or rectum.
-
Stage IVB means distant metastasis to organs such as the lungs, liver, or bones.
-
Staging guides treatment and helps predict outcome.
Questions to ask your doctor
-
What stage is my cervical cancer?
-
How large is the tumor, and how deeply has it grown into the cervix?
-
Was lymphovascular invasion present?
-
Were the surgical margins clear?
-
Were lymph nodes involved?
-
Was PD-L1 testing performed, and what do the results mean for my treatment?
We are proud to partner with:
![]()