

by Jason Wasserman MD PhD FRCPC
December 4, 2024
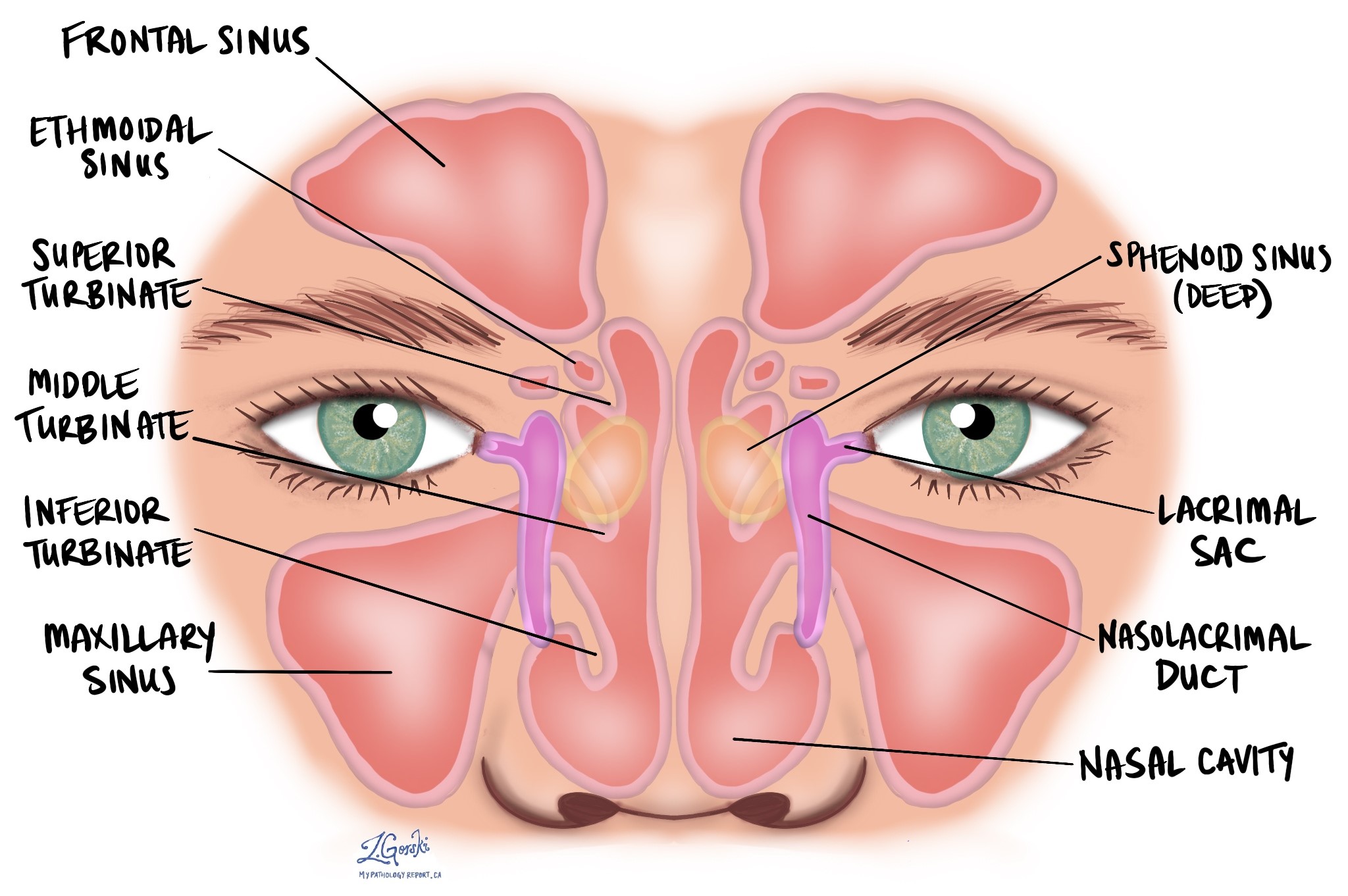
Keratinizing squamous cell carcinoma (KSCC) is a type of cancer that begins from squamous cells, specialized cells found on the inside surface of the nasal cavity and paranasal sinuses. The nasal cavity is the hollow space inside the nose that helps warm, moisten, and filter the air we breathe. The paranasal sinuses, which include the maxillary, frontal, sphenoid, and ethmoid sinuses, are air-filled spaces in the bones around the nose that lighten the weight of the skull and produce mucus to keep the nasal passages moist.
Keratinizing squamous cell carcinoma is the most common type of nasal cavity and sinus cancer and is more often seen in men. In this type of cancer, the tumour cells produce keratin, a tough protein normally found in the skin and hair. This characteristic differentiates it from a type of nasal cavity and sinus cancer called nonkeratinizing squamous cell carcinoma.
What are the symptoms of keratinizing squamous cell carcinoma?
Symptoms of keratinizing squamous cell carcinoma depend on the tumour’s size and location but may include:
- Nasal congestion or obstruction.
- Persistent nosebleeds.
- Facial pain or pressure.
- Swelling or a lump in the nasal area.
- Difficulty breathing through the nose.
- Changes in sense of smell or taste.
- Unexplained weight loss in advanced cases.
Many of these symptoms can mimic other less serious conditions, so a diagnosis often requires further testing.
What causes keratinizing squamous cell carcinoma?
Keratinizing squamous cell carcinoma can develop due to a combination of environmental, lifestyle, and biological factors:
- Occupational hazards: Prolonged exposure to certain chemicals and substances, such as nickel, chrome, arsenic, formaldehyde, welding fumes, leather dust, glues, and compounds used in textiles, is linked to the development of keratinizing squamous cell carcinoma. These occupational risks explain why the cancer is more common in men and contribute to about 30% of cases.
- Cigarette smoking: Smoking is a well-documented cause of keratinizing squamous cell carcinoma, with tobacco use significantly increasing the risk.
- Chronic inflammation: Persistent inflammation in the nasal cavity or sinuses, such as that caused by chronic sinus infections, may predispose individuals to this type of cancer.
How is this diagnosis made?
The diagnosis of keratinizing squamous cell carcinoma is typically made after a biopsy. A pathologist examines the tumour tissue under a microscope to confirm the presence of cancer and determine the subtype. Additional tests, such as imaging studies or blood tests, may be performed to assess the tumour’s size and whether it has spread.
What are the microscopic features of keratinizing squamous cell carcinoma?
Under the microscope, keratinizing squamous cell carcinoma comprises malignant epithelial cells showing squamous differentiation. This means the cells resemble the squamous cells found in normal tissues but have abnormal features.
Key characteristics include:
- Glassy, pink cytoplasm (the part of the cell surrounding the nucleus).
- Intercellular bridges (connections between cells)
- Frequent production of keratin, which may appear as small, round structures called keratin pearls
Keratinizing squamous cell carcinoma also includes several rare subtypes, such as papillary, verrucous, spindle cell, acantholytic, adenosquamous carcinoma, and carcinoma cuniculatum. Each subtype has unique features and is seen in only a few cases.

Grade
The grade of keratinizing squamous cell carcinoma describes how closely the tumour cells resemble normal squamous cells and helps predict how aggressively the cancer may grow and spread. Pathologists determine the grade by examining the tumour cells under a microscope and evaluating three key features:
- Differentiation degree: How closely the tumour cells resemble normal squamous cells. Tumours with cells that look more like normal cells are better differentiated, while those with very abnormal cells are poorly differentiated.
- Cellular pleomorphism: The variation in size and shape of the tumour cells. Tumours with more uniform cells tend to have a lower grade, while those with highly variable cells have a higher grade.
- Mitotic activity: The number of cells dividing in the tumour. Higher levels of mitotic activity indicate a more aggressive tumour and a higher grade.
Keratinizing squamous cell carcinoma is divided into three grades:
- Well differentiated keratinizing squamous cell carcinoma: The tumour cells closely resemble normal squamous cells and produce abundant keratin. This grade is uncommon.
- Moderately differentiated keratinizing squamous cell carcinoma: The cells are less like normal squamous cells and produce moderate amounts of keratin. Most keratinizing squamous cell carcinomas fall into this category.
- Poorly differentiated keratinizing squamous cell carcinoma: The cells look very abnormal and produce little keratin.
Grading provides valuable information about the tumour’s behaviour. Poorly differentiated tumours are generally more aggressive than well differentiated ones. This information is combined with other details, such as the tumour’s size and stage, to guide treatment planning.
Lymphovascular invasion
Lymphovascular invasion occurs when cancer cells invade a blood vessel or lymphatic vessel. Blood vessels are thin tubes that carry blood throughout the body, unlike lymphatic vessels, which carry a fluid called lymph instead of blood. These lymphatic vessels connect to small immune organs known as lymph nodes scattered throughout the body. Lymphovascular invasion is important because it spreads cancer cells to other body parts, including lymph nodes or the liver, via the blood or lymphatic vessels.

Perineural invasion
Pathologists use the term “perineural invasion” to describe a situation where cancer cells attach to or invade a nerve. “Intraneural invasion” is a related term that specifically refers to cancer cells inside a nerve. Nerves, resembling long wires, consist of groups of cells known as neurons. These nerves, present throughout the body, transmit information such as temperature, pressure, and pain between the body and the brain. Perineural invasion is important because it allows cancer cells to travel along the nerve into nearby organs and tissues, raising the risk of the tumour recurring after surgery.

Margins
In pathology, a margin is the edge of tissue removed during tumour surgery. The margin status in a pathology report is important as it indicates whether the entire tumour was removed or if some was left behind. This information helps determine the need for further treatment.
Pathologists typically assess margins following a surgical procedure, like an excision or resection, that removes the entire tumour. Margins aren’t usually evaluated after a biopsy, which removes only part of the tumour. The number of margins reported and their size—how much normal tissue is between the tumour and the cut edge—vary based on the tissue type and tumour location.
Pathologists examine margins to check if tumour cells are at the tissue’s cut edge. A positive margin, where tumour cells are found, suggests that some cancer may remain in the body. In contrast, a negative margin, with no tumour cells at the edge, suggests the tumour was entirely removed. Some reports also measure the distance between the nearest tumour cells and the margin, even if all margins are negative.

Lymph nodes
Small immune organs, known as lymph nodes, are located throughout the body. Cancer cells can travel from a tumour to these lymph nodes via tiny lymphatic vessels. For this reason, doctors often remove and microscopically examine lymph nodes to look for cancer cells. This process, where cancer cells move from the original tumour to another body part, like a lymph node, is termed metastasis.
Cancer cells usually first migrate to lymph nodes near the tumour, although distant lymph nodes may also be affected. Consequently, surgeons typically remove lymph nodes closest to the tumour first. They might remove lymph nodes farther from the tumour if they are enlarged and there’s a strong suspicion they contain cancer cells.

Pathologists will examine any lymph nodes removed under a microscope, and the findings will be detailed in your report. A “positive” result indicates the presence of cancer cells in the lymph node, while a “negative” result means no cancer cells were found. If the report finds cancer cells in a lymph node, it might also specify the size of the largest cluster of these cells, often referred to as a “focus” or “deposit.” Extranodal extension occurs when tumour cells penetrate the lymph node’s outer capsule and spread into the adjacent tissue.
Examining lymph nodes is important for two reasons. First, it helps determine the pathologic nodal stage (pN). Second, discovering cancer cells in a lymph node suggests an increased risk of later finding cancer cells in other body parts. This information guides your doctor in deciding whether you need additional treatments, such as chemotherapy, radiation therapy, or immunotherapy.
Pathologic staging of keratinizing squamous cell carcinoma
Staging describes the amount and location of cancer in the body. For keratinizing squamous cell carcinoma of the nasal cavity and paranasal sinuses, the staging system helps determine the size and extent of the tumour (T stage) and whether the cancer has spread to lymph nodes (N stage). This information guides treatment and helps predict outcomes.
The tumour stage (T stage) depends on where the tumour started—whether in the maxillary sinus, nasal cavity, or ethmoid sinus—as different structures and patterns of spread are associated with each location. Each site has its own staging criteria, reflecting the unique anatomy of these regions.
T stages (tumour stages)
Maxillary sinus
- Tis: The cancer is “in situ,” meaning it is confined to the surface layer and has not invaded deeper tissues.
- T1: The tumour is limited to the lining (mucosa) of the maxillary sinus and has not caused bone damage.
- T2: The tumour has caused bone damage or extends to nearby areas, such as the hard palate or middle nasal passage, but not the posterior wall of the maxillary sinus or pterygoid plates.
- T3: The tumour invades deeper areas, such as the posterior wall of the maxillary sinus, soft tissues, floor or medial wall of the eye socket (orbit), pterygoid fossa, or ethmoid sinuses.
- T4: Advanced disease, divided into:
- T4a: Moderately advanced, involving areas like the front part of the eye socket, cheek skin, or other nearby bones (cribriform plate, frontal or sphenoid sinuses).
- T4b: Very advanced, involving critical areas like the brain, cranial nerves, or skull base.
Nasal cavity and ethmoid sinus
- Tis: Cancer is “in situ,” confined to the surface layer.
- T1: The tumour is limited to one area of the nasal cavity or ethmoid sinus, with or without bone involvement.
- T2: The tumour affects two regions within the nasal cavity or ethmoid sinus or extends to adjacent areas, with or without bone involvement.
- T3: The tumour invades critical structures like the floor or medial wall of the orbit, maxillary sinus, palate, or cribriform plate.
- T4: Advanced disease, divided into:
- T4a: Moderately advanced, involving the front of the eye socket, cheek skin, minimal extension into the skull base, or nearby bones.
- T4b: Very advanced, involving the brain, cranial nerves, or deep areas of the skull.
N stages (lymph node stages)
- N0: No cancer is found in nearby lymph nodes.
- N1: Cancer is present in one lymph node on the same side of the neck, and the node is 3 cm or smaller in size without signs of spread outside the node (ENE-negative).
- N2: Cancer has spread to one or more lymph nodes, but none larger than 6 cm. It is divided into:
- N2a: A single lymph node, either 3 cm or smaller with signs of spread outside the node (ENE-positive), or larger than 3 cm but not larger than 6 cm without spread outside the node.
- N2b: Cancer in multiple lymph nodes on the same side of the neck, none larger than 6 cm, and ENE-negative.
- N2c: Cancer in lymph nodes on both sides of the neck or opposite the tumour, none larger than 6 cm, and ENE-negative.
- N3: More advanced lymph node involvement, including:
- N3a: A lymph node larger than 6 cm without spread outside the node.
- N3b: Any lymph node with spread outside the node (ENE-positive), or multiple affected lymph nodes with ENE.
Prognosis
The prognosis for keratinizing squamous cell carcinoma depends on the location of the tumour and its extent at the time of diagnosis. While the overall incidence of KSCC is decreasing, the 5-year overall survival rate is about 50%. Survival rates vary by tumour location:
- Nasal cavity: Approximately 74.5% of patients survive 5 years after diagnosis.
- Maxillary and ethmoid sinuses: The 5-year survival rate is about 35%.
- Frontal and sphenoid sinuses: Survival rates are lower, at less than 30%.
Research on certain tumour characteristics, such as the expression of PD-L1 (a protein that may affect immune system activity), suggests improved outcomes in other head and neck cancers like those in the oropharynx and larynx. Studies on PD-L1 expression in KSCC are ongoing.
If you have questions about your specific prognosis, ask your doctor to explain how these statistics apply to your situation.
We are proud to partner with:
![]()