

by Jason Wasserman MD PhD FRCPC
February 25, 2026
Mucosal melanoma of the nasal cavity and paranasal sinuses is a rare and aggressive cancer that arises from melanocytes, the cells that produce pigment (melanin), lining the nose and sinuses.
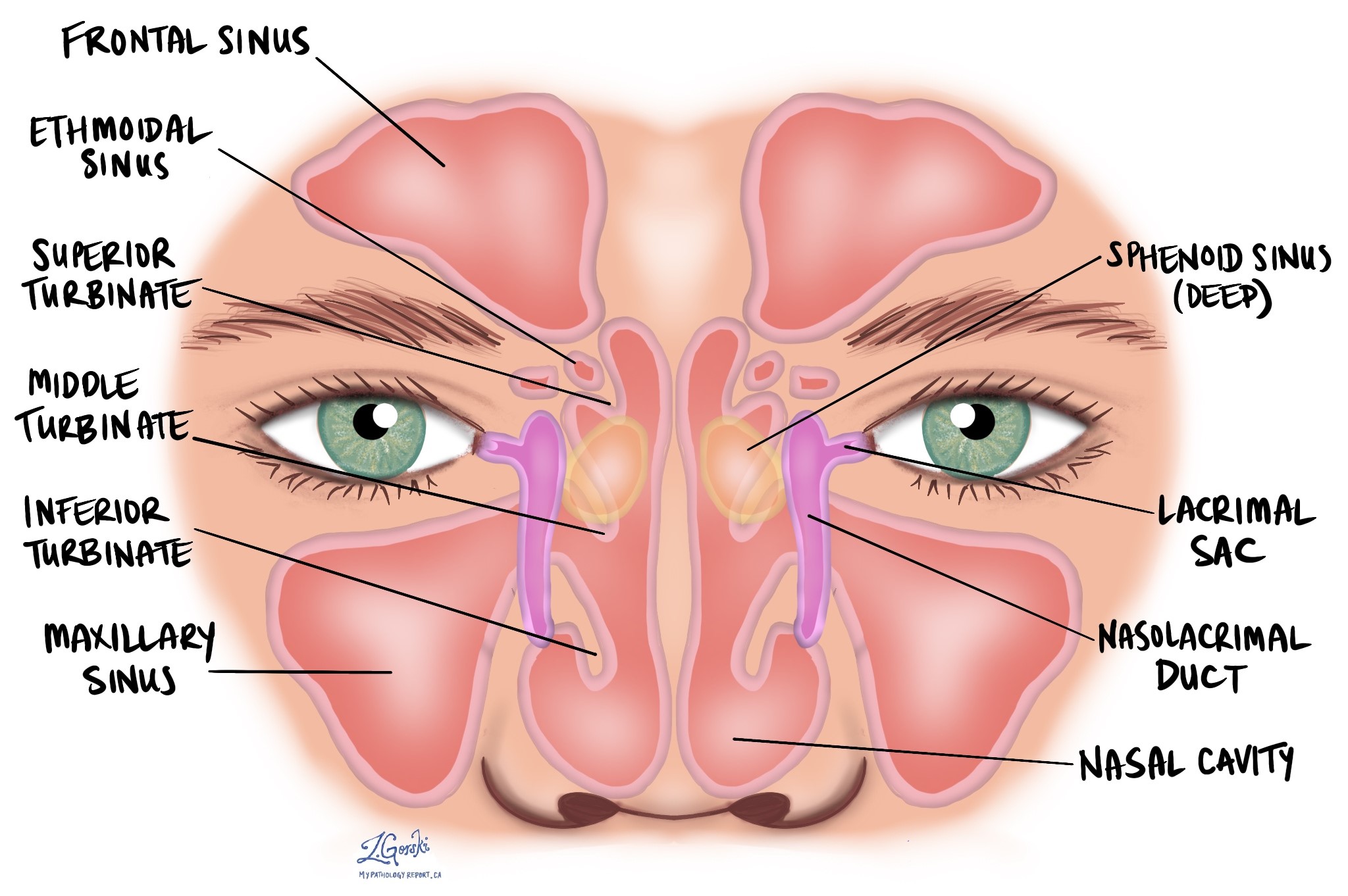
The nasal cavity is the space behind the nose through which air passes into the lungs. The paranasal sinuses are air-filled spaces in the bones around the nose, including the maxillary, ethmoid, frontal, and sphenoid sinuses.
Melanocytes are normally present in small numbers within the mucosal lining of these areas. When these cells grow uncontrollably and form a malignant tumor, the condition is called mucosal melanoma.
Unlike cutaneous melanoma, mucosal melanoma is not associated with sun exposure.
How common is mucosal melanoma in this location?
Mucosal melanoma of the head and neck is rare. About 80% of head and neck mucosal melanomas arise in the nasal cavity or maxillary sinus. However, overall, this cancer represents less than 1% of all melanomas.
It most commonly affects older adults and is uncommon in younger individuals. There is no strong evidence that it affects one sex or race more than another.
What causes mucosal melanoma?
The exact cause of mucosal melanoma of the nasal cavity and paranasal sinuses is not fully understood. Unlike cutaneous melanoma, mucosal melanoma is not associated with ultraviolet radiation. There is also no proven link to tobacco use, alcohol, chemical exposure, or viral infection.
Some tumors may arise in areas of pre-existing mucosal pigmentation (mucosal melanosis), but many develop without a clear precursor. Mucosal melanoma has a distinct genetic profile that differs from skin melanoma.
What symptoms can occur?
Symptoms of mucosal melanoma in the nasal cavity and sinuses are often nonspecific and may resemble sinus infections or inflammatory conditions. This can delay diagnosis.
Common symptoms include:
-
Nasal obstruction or congestion.
-
Recurrent nosebleeds.
-
Nasal discharge, which may be blood-stained.
-
Facial pressure or sinus discomfort.
On endoscopic examination, the tumor may appear as a fleshy, polyp-like mass. It may be darkly pigmented, but up to half of tumors lack visible pigment and may appear pink or gray.
In some cases, patients may have enlarged lymph nodes at the time of diagnosis. Distant spread may also be present.
How is this diagnosis made?
The diagnostic process usually begins when a suspicious mass is identified during nasal endoscopy or imaging. A biopsy of the abnormal tissue is performed, and the diagnosis is made after microscopic examination by a pathologist.
The diagnosis is confirmed when malignant cells show evidence of melanocytic differentiation, meaning they produce melanin or express melanocyte-related proteins.
Microscopic features
Under the microscope, mucosal melanoma shows highly atypical tumor cells that may vary in shape. The cells may be epithelioid (large and polygonal), spindle-shaped, round, clear, plasmacytoid, or undifferentiated. More than one cell type is often present within the same tumor.
The tumor may grow in sheets, nests, or bundles of elongated cells. Invasion into the underlying connective tissue is common. Advanced tumors may invade cartilage or bone.
The surface lining may show abnormal melanocytes spreading upward within the epithelium (pagetoid spread) or arranged along the basal layer (lentiginous growth). Mitotic figures are usually numerous and may appear abnormal. Areas of necrosis are common.
Up to 50% of tumors may lack visible pigment (amelanotic melanoma), making diagnosis more challenging.
Immunohistochemistry
Immunohistochemistry is a laboratory test that uses antibodies to detect specific proteins within tumor cells. This test is especially important in amelanotic tumors.
Tumor cells in mucosal melanoma typically express melanocytic markers, including S100, SOX10, HMB45, Melan-A (MART1), tyrosinase, and MITF. Because no single marker is completely sensitive, a panel of markers is used. These tests help distinguish mucosal melanoma from other cancers that can appear similar.
Imaging studies
Imaging studies are used to determine how far the tumor has spread locally and whether it has spread to lymph nodes or distant organs.
A CT scan helps identify bone destruction and is important for surgical planning.
An MRI scan provides better detail of soft tissues and is particularly useful for assessing invasion into the orbit (eye socket), brain, or surrounding structures. MRI with contrast is the preferred imaging method for detecting brain metastases.
PET-CT may be performed to evaluate lymph nodes and detect distant metastases. Mucosal melanomas are often highly active on PET imaging.
Imaging findings are combined with pathology results to determine tumor stage and guide treatment planning.
Subtypes of mucosal melanoma
A subtype is a specific form of a cancer that shares the main features of the overall disease but has distinct microscopic characteristics. Identifying a subtype can provide additional information about tumor behavior.
Mucosal lentiginous melanoma
This subtype shows abnormal melanocytes spreading linearly along the basal layer of the epithelium. This growth pattern is common in sinonasal melanoma.
Nodular melanoma
This subtype forms a more compact, nodular mass and may show minimal surface involvement (in situ). It is often deeply invasive at the time of diagnosis.
Desmoplastic mucosal melanoma
This rare subtype consists mainly of spindle-shaped tumor cells within dense fibrous tissue. It may lack visible pigment and can resemble other spindle cell tumors. Perineural invasion is frequently present. Extensive immunohistochemical testing is often required for diagnosis.
Depth of invasion
Depth of invasion describes how far the tumor has grown into surrounding tissues.
Under the microscope, pathologists assess how deeply the tumor extends beneath the surface lining and whether it invades cartilage, bone, or nearby structures. Imaging studies such as CT and MRI also help evaluate the extent of local invasion.
However, unlike in cutaneous melanoma, tumor thickness (Breslow depth) is not used to stage mucosal melanoma. Most mucosal melanomas of the head and neck are considered advanced (T3 or T4) at diagnosis under current staging systems because of their aggressive behavior.
Therefore, while the depth of invasion is documented, the overall stage depends more on local extension and spread to lymph nodes or distant organs.
Lymph nodes and nodal stage
Lymph nodes are small immune organs connected by lymphatic vessels. Cancer cells can spread to lymph nodes through these vessels.
Lymph nodes may be evaluated by imaging, biopsy, or surgical removal. In the pathology report, lymph nodes are described as:
-
Positive, if cancer cells are present.
-
Negative, if no cancer cells are found.
The number of positive lymph nodes helps determine nodal stage. Lymph node involvement is associated with a higher risk of distant spread and a poorer prognosis.
At diagnosis, approximately 20% of patients may have lymph node metastases.
Perineural invasion
Perineural invasion (PNI) means cancer cells are seen growing along or around a nerve. This is common in mucosal melanoma and is considered a high-risk feature because it indicates aggressive local spread.
Biomarkers
Biomarkers are proteins or genetic changes found in tumor cells that may help guide treatment decisions. In mucosal melanoma of the nasal cavity and paranasal sinuses, biomarker testing is most often performed in advanced or metastatic disease to identify potential targeted therapy or immunotherapy options.
KIT
KIT is a gene that regulates cell growth. Mutations in KIT are more common in mucosal melanoma than in skin melanoma. If a KIT mutation is identified through molecular testing, targeted therapy directed at KIT may be considered.
KIT mutations are detected using molecular genetic testing on tumor tissue. Results are reported as either a detectable mutation or no mutation identified. The specific mutation may be described.
BRAF
BRAF is a gene involved in cell signaling. BRAF mutations are less common in mucosal melanoma than in cutaneous melanoma. If present, certain targeted therapies may be effective.
BRAF mutations are identified using molecular testing. The report will indicate whether a mutation is present and may specify the type.
PD-L1
PD-L1 is a protein that helps cancer cells avoid detection by the immune system. Tumors expressing PD-L1 may respond better to immunotherapy.
PD-L1 is tested using immunohistochemistry. Results are typically reported as the percentage of tumor cells showing staining or using a scoring system. Higher expression may increase the likelihood of response to immune checkpoint inhibitors.
Prognosis
Mucosal melanoma of the nasal cavity and paranasal sinuses is an aggressive cancer. The 5-year overall survival rate ranges from approximately 20% to 50%.
Prognosis depends on tumor size, extent of local invasion, lymph node involvement, and distant metastasis. Tumors confined to the nasal cavity may have better outcomes than those involving deeper sinus structures.
Surgical removal is the primary treatment. Radiation therapy may improve local control. Targeted therapy and immunotherapy may be considered in advanced cases.
Questions to ask your doctor
-
Has the tumor spread to lymph nodes or distant organs?
-
Has it invaded nearby structures such as the bone or the orbit?
-
Were biomarker tests performed?
-
Am I a candidate for targeted therapy or immunotherapy?
-
What stage am I in, and what does that mean for my treatment?
We are proud to partner with:
![]()