

by Jason Wasserman MD PhD FRCPC
January 24, 2024
Low grade fibromyxoid sarcoma (also known as Evan’s tumour) is a rare type of soft tissue cancer. As its name suggests, low grade fibromyxoid sarcoma is typically considered a low grade sarcoma, meaning it tends to grow and spread more slowly compared to high grade tumours. However, it has a potential for late recurrence and metastasis, and thus, long-term follow-up is essential.
Where in the body is low grade fibromyxoid sarcoma normally found?
This tumour typically involves the deep soft tissues, often developing in the trunk, arms, or legs, but it can occur anywhere in the body.
What are the symptoms of low grade fibromyxoid sarcoma?
The symptoms of low grade fibromyxoid sarcoma can be quite subtle and generally depend on the tumour’s location. The most common symptom is a painless, slowly growing lump or mass. Because it grows slowly, it might take a while before it’s noticed or causes any discomfort. If the tumour presses against nerves or muscles, it may cause pain or difficulty in movement.
What causes low grade fibromyxoid sarcoma?
The exact cause of low grade fibromyxoid sarcoma is not clearly understood. As with many cancers, it appears to result from changes in the body’s cells that lead to uncontrolled growth. However, these changes are usually not inherited but occur spontaneously.
What genetic changes are found in low grade fibromyxoid sarcoma?
Low grade fibromyxoid sarcoma is associated with a specific genetic change known as a chromosomal rearrangement. This involves the fusion of part of chromosome 7 (7q33) with chromosome 16 (16p11), resulting in the FUS-CREB3L2 gene fusion. This fusion is believed to play a key role in the development of the tumour.
How is this diagnosis made?
Diagnosing low grade fibromyxoid sarcoma involves a combination of medical imaging, such as MRI or CT scans, and a biopsy. The imaging tests can identify the presence of a mass, while a biopsy, where a sample of the tumour is taken and examined under a microscope, is crucial for confirming the diagnosis.
Your pathology report for low grade fibromyxoid sarcoma
The information found in your pathology report for low grade fibromyxoid sarcoma will depend on the type of procedure performed. For example, the information found in a report after a biopsy is performed is usually limited to the diagnosis although some reports may also describe the results of additional tests such as immunohistochemistry (IHC), fluorescence in situ hybridization (FISH), or next-generation sequencing (NGS). After the entire tumour has been removed, your pathology report will include additional information such as the presence or absence of lymphovascular and perineural invasion, treatment effect, and the assessment of margins. The results of any lymph nodes examined should also be included in this final report. These topics are described in more detail in the sections below.
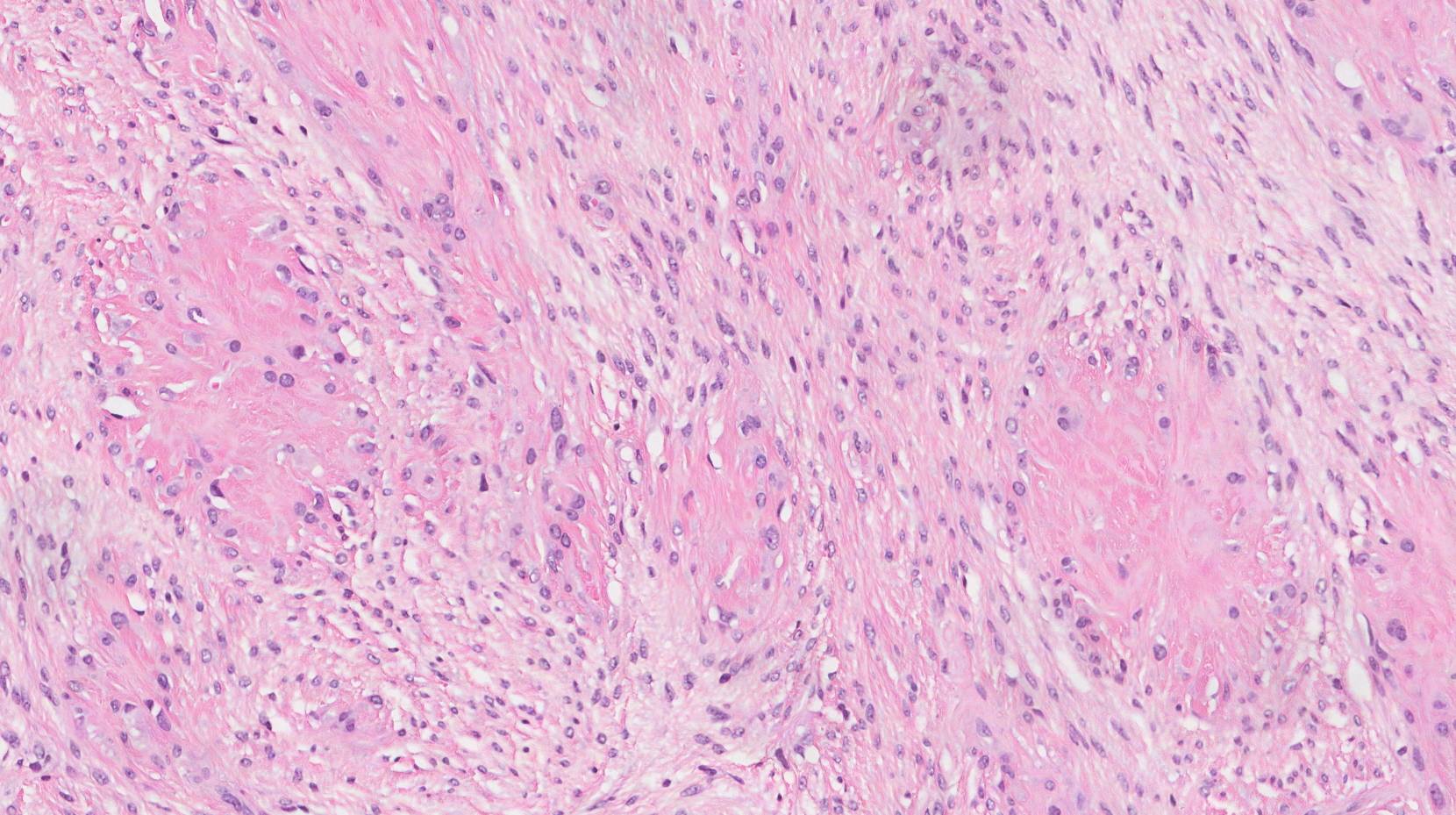
Microscopic features
Under the microscope, low grade fibromyxoid sarcoma shows distinct features. It’s characterized by a mix of fibrous and myxoid areas – the fibrous areas being more collagen-rich and the myxoid areas being more gel-like. The cells usually appear spindle-shaped and are arranged in a swirling or whorled pattern.
Additional tests
Immunohistochemistry
Immunohistochemistry (IHC) involves using special stains (antibodies) that react with specific proteins in the tumour cells. In the case of low grade fibromyxoid sarcoma, this test can highlight certain proteins that are typically found in the tumour cells, helping to distinguish low grade fibromyxoid sarcoma from other types of tumours that can look similar when examined under the microscope.
- MUC4 Expression: One of the most significant markers for low grade fibromyxoid sarcoma is the MUC4 protein. The presence of MUC4 is a key diagnostic feature, as it is consistently expressed in low grade fibromyxoid sarcoma. MUC4 is a high molecular weight glycoprotein, and its detection in tissue samples of suspected low grade fibromyxoid sarcoma is highly suggestive of this diagnosis.
Other Markers: While MUC4 is a primary marker, low grade fibromyxoid sarcoma may also express other proteins, but these are not as definitive or specific as MUC4. These can include:
- EMA (epithelial membrane antigen): Low grade fibromyxoid sarcoma may show focal positivity for EMA.
- SMA (smooth muscle actin): Occasionally, low grade fibromyxoid sarcoma cells may express SMA, but this is not a consistent finding.
Negative markers: Low grade fibromyxoid sarcoma typically does not express certain markers that are found in other types of soft tissue tumours. For instance, it usually does not express S100 protein, desmin, or CD34, helping to differentiate it from other sarcomas.
The immunohistochemical profile of low grade fibromyxoid sarcoma, especially the presence of MUC4, is an important tool for pathologists in diagnosing this rare and often challenging-to-identify tumour. The use of IHC not only aids in confirming the diagnosis of low grade fibromyxoid sarcoma but also helps in distinguishing it from other soft tissue tumours with similar histological features.
Molecular tests
In some situations, molecular tests such as next-generation sequencing (NGS) or fluorescence in situ hybridization (FISH) will also be performed. These tests look for the specific FUS-CREB3L2 gene fusion, thereby confirming the diagnosis of low grade fibromyxoid sarcoma.
Tumour grade
Pathologists divide low grade fibromyxoid sarcoma into three grades based on a system created by the French Federation of Cancer Centers Sarcoma Group (FNCLCC). This system uses three microscopic features to determine the tumour grade: differentiation, mitotic count, and necrosis. These features are explained in more detail below. The grade can only be determined after a sample of the tumour has been examined under the microscope.
Points (from 0 to 3) are assigned for each of the microscopic features (0 to 3) and the total number of points determines the final grade of the tumour. According to this system, synovial sarcomas may be either low or high-grade tumours. High grade tumours (grades 2 and 3) are associated with a worse prognosis. As its name suggests, the vast majority of low grade fibromyxoid sarcomas are considered “low grade” according to this system.
Points associated with each grade:
- Grade 1 – 2 or 3 points.
- Grade 2 – 4 or 5 points.
- Grade 3 – 6 to 8 points.
Microscopic features used to determine the grade:
- Tumour differentiation – Tumour differentiation describes how closely the tumour cells look like normal healthy cells. Tumour cells that look very similar to normal cells are given 1 point while those that look nothing like normal cells are given 3 points. All low grade fibromyxoid sarcomas are given 1 point for tumour differentiation.
- Mitotic count – A cell that is in the process of dividing to create two new cells is called a mitotic figure. Tumours that are growing fast tend to have more mitotic figures than tumours that are growing slowly. Your pathologist will determine the mitotic count by counting the number of mitotic figures in ten areas of the tumour while looking through the microscope. Tumours with no mitotic figure or very few mitotic figures are given 1 point while those with 10 to 20 mitotic figures are given 2 points and those with more than 20 mitotic figures are given 3 points.
- Necrosis – Necrosis is a type of cell death. Tumours that are growing fast tend to have more necrosis than tumours that are growing slowly. If your pathologist sees no necrosis, the tumour will be given 0 points. The tumour will be given 1 point if necrosis is seen but makes up less than 50% of the tumour or 2 points if necrosis makes more than 50% of the tumour.
Treatment effect
If you received chemotherapy and/or radiation therapy before the operation to remove the tumour, your pathologist will examine all the tissue sent to pathology to see how much of the tumour was still alive at the time it was removed from the body. Pathologists use the term viable to describe tissue that was still alive at the time it was removed from the body. In contrast, pathologists use the term non-viable to describe tissue that was not alive at the time it was removed from the body. Most commonly, your pathologist will describe the percentage of tumours that is non-viable.
Perineural invasion
Pathologists use the term “perineural invasion” to describe a situation where cancer cells attach to or invade a nerve. “Intraneural invasion” is a related term that specifically refers to cancer cells found inside a nerve. Nerves, resembling long wires, consist of groups of cells known as neurons. These nerves, present throughout the body, transmit information such as temperature, pressure, and pain between the body and the brain. The presence of perineural invasion is important because it allows cancer cells to travel along the nerve into nearby organs and tissues, raising the risk of the tumour recurring after surgery.

Lymphovascular invasion
Lymphovascular invasion occurs when cancer cells invade a blood vessel or lymphatic channel. Blood vessels, thin tubes that carry blood throughout the body, contrast with lymphatic channels, which carry a fluid called lymph instead of blood. These lymphatic channels connect to small immune organs known as lymph nodes, scattered throughout the body. Lymphovascular invasion is important because it enables cancer cells to spread to other body parts, including lymph nodes or the lungs, via the blood or lymphatic vessels.

Margins
In pathology, a margin refers to the edge of tissue removed during tumour surgery. The margin status in a pathology report is important as it indicates whether the entire tumour was removed or if some was left behind. This information helps determine the need for further treatment.
Pathologists typically assess margins following a surgical procedure like an excision or resection, aimed at removing the entire tumour. Margins aren’t usually evaluated after a biopsy, which removes only part of the tumour. The number of margins reported and their size—how much normal tissue is between the tumour and the cut edge—vary based on the tissue type and tumour location.
Pathologists examine margins to check if tumour cells are present at the tissue’s cut edge. A positive margin, where tumour cells are found, suggests that some cancer may remain in the body. In contrast, a negative margin, with no tumour cells at the edge, suggests the tumour was fully removed. Some reports also measure the distance between the nearest tumour cells and the margin, even if all margins are negative.

Lymph nodes
Lymph nodes are small immune organs found throughout the body. Cancer cells can spread from a tumour to lymph nodes through small lymphatic vessels. For this reason, lymph nodes are commonly removed and examined under a microscope to look for cancer cells. The movement of cancer cells from the tumour to another part of the body such as a lymph node is called a metastasis.
Cancer cells typically spread first to lymph nodes close to the tumour although lymph nodes far away from the tumour can also be involved. For this reason, the first lymph nodes removed are usually close to the tumour. Lymph nodes further away from the tumour are only typically removed if they are enlarged and there is a high clinical suspicion that there may be cancer cells in the lymph node.
If any lymph nodes were removed from your body, they will be examined under the microscope by a pathologist and the results of this examination will be described in your report. “Positive” means that cancer cells were found in the lymph node. “Negative” means that no cancer cells were found. If cancer cells are found in a lymph node, the size of the largest group of cancer cells (often described as “focus” or “deposit”) may also be included in your report. Extranodal extension means that the tumour cells have broken through the capsule on the outside of the lymph node and have spread into the surrounding tissue.
The examination of lymph nodes is important for two reasons. First, this information is used to determine the pathologic nodal stage (pN). Second, finding cancer cells in a lymph node increases the risk that cancer cells will be found in other parts of the body in the future. As a result, your doctor will use this information when deciding if additional treatment such as chemotherapy, radiation therapy, or immunotherapy is required.

Pathologic stage
The pathologic stage for low grade fibromyxoid sarcoma is based on the TNM staging system, an internationally recognized system created by the American Joint Committee on Cancer. This system uses information about the primary tumour (T), lymph nodes (N), and distant metastatic disease (M) to determine the complete pathologic stage (pTNM). Your pathologist will examine the tissue submitted and give each part a number. In general, a higher number means a more advanced disease and a worse prognosis.
Tumour stage (pT)
The tumour stage for low grade fibromyxoid sarcoma varies based on the body part involved. For example, a 5-centimetre tumour that starts in the head will be given a different tumour stage than a tumour that starts deep in the back of the abdomen (the retroperitoneum). However, in most body sites, the tumour stage includes the tumour size and whether the tumour has grown into surrounding body parts.
Head and neck
- T1 – The tumour is no greater than 2 centimetres in size.
- T2 – The tumour is between 2 and 4 centimetres in size.
- T3 – The tumour is greater than 4 centimetres in size.
- T4 – The tumour has grown into surrounding tissues such as the bones of the face or skull, the eye, the larger blood vessels in the neck, or the brain.
Chest, back, or stomach and the arms or legs (trunk and extremities)
- T1 – The tumour is no greater than 5 centimetres in size.
- T2 – The tumour is between 5 and 10 centimetres in size.
- T3 – The tumour is between 10 and 15 centimetres in size.
- T4 – The tumour is greater than 15 centimetres in size.
Abdomen and organs inside the chest (thoracic visceral organs)
- T1 – The tumour is only seen in one organ.
- T2 – The tumour has grown into the connective tissue that surrounds the organ from which it started.
- T3 – The tumour has grown into at least one other organ.
- T4 – Multiple tumours are found.
Retroperitoneum (the space at the very back of the abdominal cavity)
- T1 – The tumour is no greater than 5 centimetres in size.
- T2 – The tumour is between 5 and 10 centimetres in size.
- T3 – The tumour is between 10 and 15 centimetres in size.
- T4 – The tumour is greater than 15 centimetres in size.
Tissue around the eye (orbit)
- T1 – The tumour is no greater than 2 centimetres in size.
- T2 – The tumour is greater than 2 centimetres in size but has not grown into the bones surrounding the eye.
- T3 – The tumour has grown into the bones surrounding the eye or other bones of the skull.
- T4 – The tumour has grown into the eye (the globe) or the surrounding tissues such as the eyelids, sinuses, or brain.
Nodal stage (pN)
Low grade fibromyxoid sarcoma is given a nodal stage of 0 or 1 based on the presence or absence of tumour cells in one or more lymph nodes. If no tumour cells are seen in any lymph nodes, the nodal stage is N0. If no lymph nodes are sent for pathological examination, the nodal stage cannot be determined, and the nodal stage is listed as NX. If tumour cells are found in any lymph nodes, then the nodal stage is listed as N1.
Other helpful resources
Atlas of Pathology
We are proud to partner with:
![]()