

by Jason Wasserman MD PhD FRCPC
February 16, 2026
Oral epithelial dysplasia is a precancerous condition affecting the lining of the oral cavity, including the mouth, tongue, and lips. It develops in the epithelium, the thin surface layer of cells that covers the inside of the mouth and serves as a protective barrier.
In oral epithelial dysplasia, epithelial cells grow and mature abnormally. These cells may appear irregular in size and shape, may divide more frequently than normal, and may lose their usual orderly arrangement. These microscopic changes reflect damage to the cells’ genetic material and reduced control over normal growth. Although oral epithelial dysplasia is not cancer, it is important because these abnormal cells have the potential to progress to squamous cell carcinoma, the most common type of cancer of the oral cavity.
Where in the oral cavity does oral epithelial dysplasia usually occur?
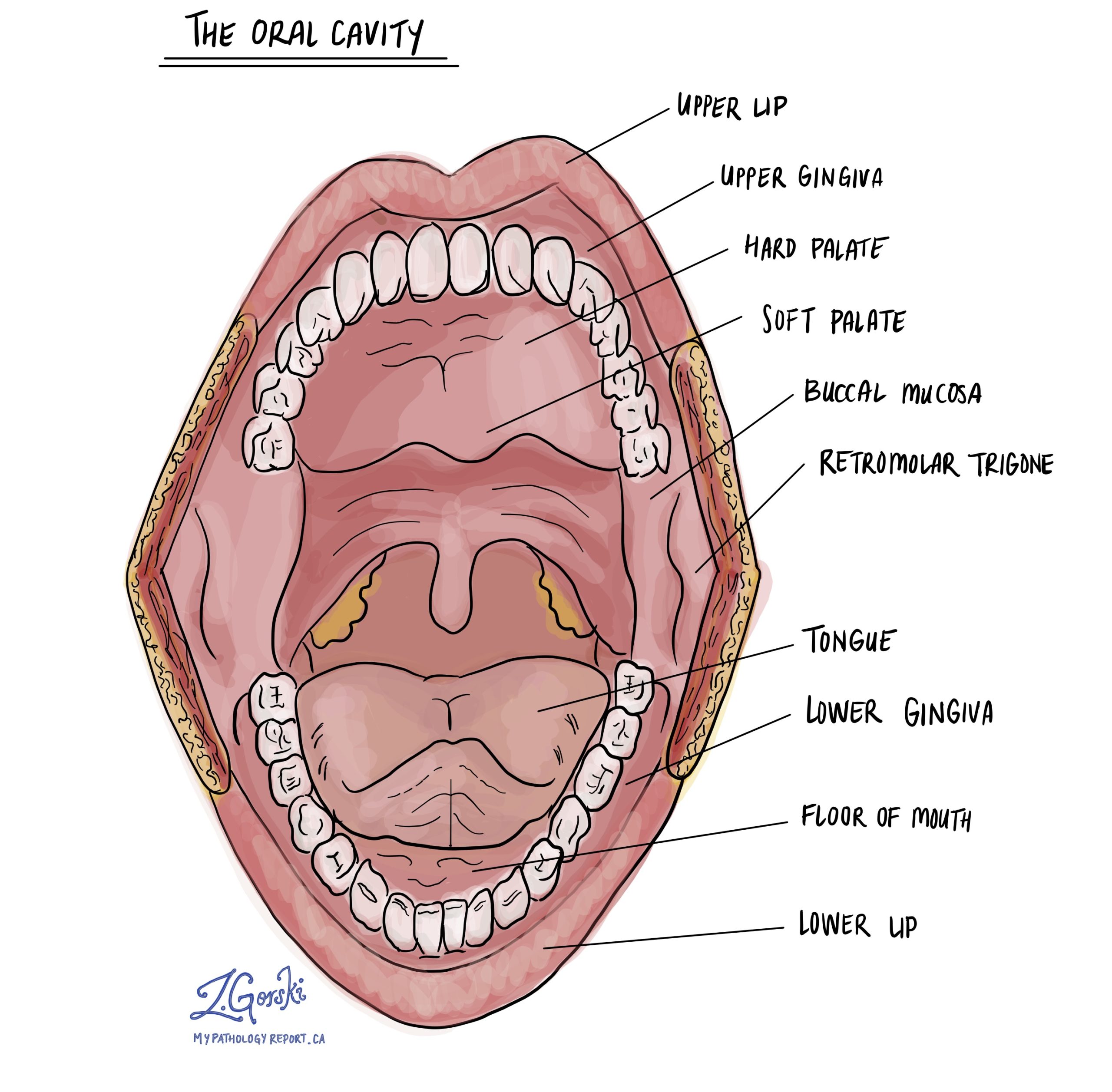
Oral epithelial dysplasia can develop in any part of the oral cavity that is lined by squamous epithelium. It most often affects areas that are more vulnerable to chronic irritation or exposure to harmful substances. These commonly include the tongue, particularly the sides and underside; the floor of the mouth beneath the tongue; the inner lining of the cheeks; the gums; the hard palate, which forms the roof of the mouth; and the inner surface of the lips.
What are the symptoms of oral epithelial dysplasia?
Many people with oral epithelial dysplasia have no symptoms, especially in the early stages. When symptoms do occur, they often develop slowly and may be subtle. Patients may notice persistent white or red patches, or areas that appear thicker, rougher, or different in texture from the surrounding tissue. Some individuals experience pain, tenderness, or increased sensitivity in the affected area, particularly when eating spicy, acidic, or hot foods.
If a larger area of the oral cavity is involved, oral epithelial dysplasia may interfere with normal oral function. This can lead to difficulty chewing or swallowing. In some cases, people report numbness or altered sensation in the affected region. Because these changes can resemble other noncancerous conditions, oral epithelial dysplasia is often discovered during a routine dental examination or after a biopsy.
What causes oral epithelial dysplasia?
Oral epithelial dysplasia develops as a result of ongoing damage to the cells lining the oral cavity. One of the most important risk factors is tobacco use, including cigarettes, cigars, pipes, and smokeless tobacco products. Alcohol use also increases the risk, particularly when combined with tobacco, because alcohol can weaken the protective lining of the mouth and allow harmful substances to penetrate more easily.
Chronic irritation and inflammation can also contribute to the development of oral epithelial dysplasia. This includes conditions such as oral lichen planus or long-standing mechanical irritation from poorly fitting dental appliances. Immune suppression is another important factor. People taking immune-suppressing medications or those who have undergone an organ transplant are at increased risk because their immune systems are less able to recognize and remove abnormal cells.
In some regions of the world, chewing betel (areca) nut is a major cause of oral epithelial dysplasia. Betel nut contains compounds that directly damage epithelial cells and promote abnormal growth. It is important to note that not everyone with these risk factors develops dysplasia, and some cases occur without a clearly identifiable cause.
How is oral epithelial dysplasia diagnosed?
Oral epithelial dysplasia is diagnosed by examining a biopsy, which is a small tissue sample taken from the abnormal area in the mouth. A pathologist examines the tissue under a microscope to assess how abnormal the epithelial cells appear, how well they are organized, and how much of the epithelial thickness is involved by abnormal changes.
Based on these microscopic findings, the pathologist assigns a grade to the dysplasia. The grade provides important information about the risk of cancer progression and helps guide decisions about treatment and follow-up.
How is oral epithelial dysplasia graded?
Oral epithelial dysplasia is commonly classified as low-grade or high-grade based on the severity of abnormal cell changes and the extent of involvement of the epithelial lining.
In low-grade oral epithelial dysplasia, the abnormal changes are mild and are usually confined to the lower portion of the epithelium. The risk of progression to cancer is relatively low, although it is not zero. Management often involves careful clinical monitoring, repeat examinations, and follow-up biopsies if the lesion changes over time.
In high-grade oral epithelial dysplasia, the abnormal cells show more pronounced changes and involve a larger portion of the epithelial thickness. This grade is associated with a significantly higher risk of progression to squamous cell carcinoma. Because of this increased risk, treatment often includes surgical removal of the affected tissue when possible, along with close follow-up.
Is oral epithelial dysplasia cancer?
Oral epithelial dysplasia is not cancer, but it is considered a precancerous condition. This means that the abnormal cells have the potential to develop into cancer over time. The likelihood of progression depends on the grade of dysplasia, the presence of ongoing risk factors such as tobacco or alcohol use, and whether the lesion is treated or closely monitored. High-grade dysplasia carries a greater risk of developing into oral cavity cancer than low-grade dysplasia.
Why is early detection important?
Early detection of oral epithelial dysplasia allows doctors to intervene before cancer develops. Identifying and monitoring low-grade lesions can help detect progression at an early stage, while treating high-grade lesions can significantly reduce the risk of invasive cancer. Regular dental examinations and prompt evaluation of any persistent changes in the mouth are key to early diagnosis and effective management.
Questions you may want to ask your doctor
If you have been diagnosed with oral epithelial dysplasia, you may wish to ask your doctor:
-
What grade of oral epithelial dysplasia was found in my biopsy?
-
What is my personal risk of developing oral cancer?
-
Should this area be removed, or can it be safely monitored?
-
How often should I have follow-up examinations or repeat biopsies?
-
Are there lifestyle changes, such as quitting tobacco or reducing alcohol use, that could lower my risk?
We are proud to partner with:
![]()