

by Jason Wasserman MD PhD FRCPC
January 27, 2026
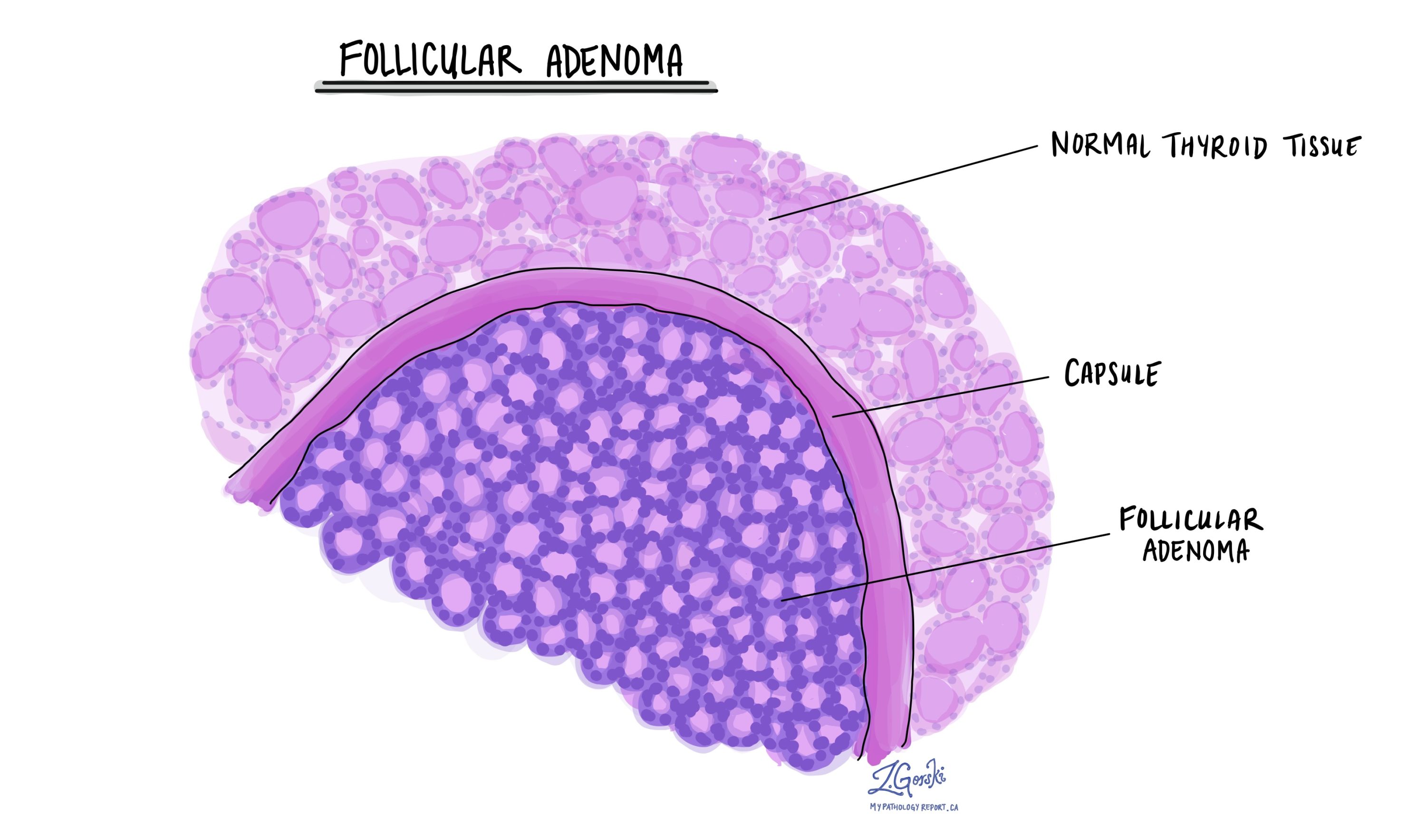
Follicular adenoma is a benign (noncancerous) tumour of the thyroid gland. It develops from follicular cells, the normal cells that produce thyroid hormone.
A capsule surrounds this tumour, and the tumour does not invade nearby thyroid tissue, blood vessels, or lymphatic channels. It also lacks the nuclear features of papillary thyroid carcinoma, an essential distinction from thyroid cancer.
This article explains how follicular thyroid adenoma is diagnosed, what pathologists look for under the microscope, and how this diagnosis helps explain the findings in your pathology report.
Where does follicular thyroid adenoma occur?
Follicular thyroid adenomas can arise anywhere within the thyroid gland. Rarely, they can develop in ectopic thyroid tissue, meaning thyroid tissue located outside the normal gland. Examples include thyroglossal duct cysts, lingual thyroid tissue at the base of the tongue, and ovarian thyroid tissue (struma ovarii).
What are the symptoms of follicular thyroid adenoma?
Most people with follicular thyroid adenoma have no symptoms. The tumour is often discovered during a routine physical examination or incidentally on imaging studies performed for other reasons. Some patients notice a painless lump in the neck. Larger tumours can press on nearby structures and cause difficulty swallowing, shortness of breath, or a sensation of pressure in the neck.
Most patients have normal thyroid hormone levels. In rare cases, a follicular adenoma may produce excess thyroid hormone and cause symptoms of hyperthyroidism.
What causes follicular thyroid adenoma?
Most follicular thyroid adenomas occur sporadically, meaning there is no identifiable cause. However, childhood exposure to radiation involving the head and neck is a well-established risk factor. Iodine deficiency has also been associated with the development of these tumours.
In some patients, follicular thyroid adenoma occurs as part of an inherited tumour syndrome, particularly when adenomas are multiple, occur at a young age, or are found alongside numerous other thyroid nodules. Examples include PTEN hamartoma tumour syndrome (such as Cowden syndrome), DICER1 syndrome, and Carney complex. In these situations, further clinical or genetic evaluation may be recommended.
How is this diagnosis made?
The diagnosis of follicular thyroid adenoma is made through a combination of imaging, biopsy, surgical removal, and careful examination by a pathologist.
Imaging
Ultrasound usually shows a single, well-defined thyroid nodule, often with a surrounding halo that represents the tumour capsule. Imaging alone cannot reliably distinguish a follicular thyroid adenoma from a follicular thyroid carcinoma, as both can appear very similar.
Fine needle aspiration biopsy
A fine needle aspiration biopsy may show a follicular-patterned lesion and is often reported as a “follicular neoplasm” or “suspicious for follicular neoplasm.” This result does not indicate cancer. Notably, follicular adenoma and follicular carcinoma cannot be distinguished on biopsy alone because the diagnosis depends on whether the tumour invades its capsule or blood vessels.
Surgical removal and pathology examination
A definitive diagnosis is made after the tumour is surgically removed. The pathologist examines the entire tumour and its capsule under the microscope to specifically assess capsular or vascular invasion. The absence of both confirms the diagnosis of follicular thyroid adenoma.
Microscopic features
When examined under the microscope, follicular thyroid adenoma is a well-encapsulated tumour composed of follicle-forming cells. The follicles may be small, medium, or large, and the overall growth pattern can vary. The tumour cells resemble normal thyroid follicular cells and have round nuclei with smooth contours.
Crucially, no capsular invasion is observed, indicating that the tumour cells do not grow through the capsule into surrounding thyroid tissue. No vascular invasion is identified, indicating that tumour cells are not found within blood vessels. The nuclear features characteristic of papillary thyroid carcinoma are absent. Cell division is minimal, and tumour cell death (necrosis) is not present.
Because invasion can be very focal, the capsule is often examined extensively, sometimes with additional tissue sections, to be certain that no invasion is present.
Immunohistochemistry
Immunohistochemistry uses special stains to confirm the thyroid origin of the tumour. Follicular thyroid adenomas typically express thyroglobulin, thyroid transcription factor 1 (TTF-1), and PAX8, all of which are normal markers of thyroid follicular cells. The proliferation index (Ki-67) is low, reflecting the tumour’s slow growth.
There are no immunohistochemical stains that can reliably distinguish follicular thyroid adenoma from follicular thyroid carcinoma. The diagnosis still depends on identifying the absence of invasion.
Molecular testing
Molecular testing is not required to diagnose follicular thyroid adenoma, but it may be performed in some cases. Specific genetic changes, such as RAS mutations or PAX8–PPARG rearrangements, are found in follicular adenomas and some thyroid cancers. Because of this overlap, molecular results alone are not used to determine whether a tumour is benign or malignant. Instead, they may provide supportive information in selected or challenging cases.
Prognosis
Follicular thyroid adenoma is a benign tumour with an excellent prognosis. When the tumour is completely removed, it does not spread to lymph nodes or other organs and does not recur. No additional cancer treatment is required after surgery, and long-term outcomes are excellent. Follow-up care is typically focused on routine thyroid monitoring rather than cancer surveillance.
Questions to ask your doctor
-
Do I need ongoing thyroid hormone monitoring?
-
Is there any concern for an inherited condition based on my findings?
-
Will I need follow-up imaging or blood tests?
We are proud to partner with:
![]()