

by Jason Wasserman MD PhD FRCPC
May 13, 2026
Follicular adenoma is a benign (noncancerous) tumor of the thyroid gland. The thyroid is a butterfly-shaped gland at the front of the neck that produces hormones to regulate metabolism. Follicular adenoma develops from follicular cells, which normally produce thyroid hormone.
The tumor is completely surrounded by a thin layer of tissue called a capsule, and the tumor cells do not invade the surrounding thyroid tissue, blood vessels, or lymphatic channels. The absence of invasion is what distinguishes follicular adenoma from follicular thyroid carcinoma, the cancerous counterpart of this tumor. Follicular adenoma also lacks the specific nuclear changes (the part of the cell that contains genetic material) seen in papillary thyroid carcinoma, the most common type of thyroid cancer.
Where does a follicular adenoma occur?
Follicular adenomas can develop anywhere within the thyroid gland. Rarely, they can arise in thyroid tissue located outside the normal gland, called ectopic thyroid tissue. Examples include a thyroglossal duct cyst (a developmental remnant in the neck), lingual thyroid tissue at the base of the tongue, or struma ovarii (thyroid tissue found within an ovarian teratoma). When this happens, the tumor still looks and behaves like a follicular adenoma but in an unusual location.
What are the symptoms of a follicular adenoma?
Most people with follicular adenoma have no symptoms. The tumor is often discovered during a routine physical examination or by chance on imaging done for another reason. Some people notice a painless lump in the neck. Larger tumors can press on nearby structures, causing difficulty swallowing, shortness of breath, or a sensation of pressure in the neck.
Most patients have normal thyroid hormone levels. In rare cases, a follicular adenoma produces excess thyroid hormone and causes symptoms of hyperthyroidism (an overactive thyroid), such as weight loss, a fast heartbeat, heat intolerance, or anxiety.
What causes follicular adenoma?
Most follicular adenomas occur on their own (sporadically), with no identifiable cause. Known risk factors include:
- Radiation exposure during childhood. Previous radiation involving the head and neck increases the risk of all thyroid tumors, including follicular adenoma.
- Iodine deficiency. Iodine is needed to make thyroid hormone. A low-iodine diet has been associated with the development of follicular tumors.
- Inherited tumor syndromes. In some patients, a follicular adenoma is part of an inherited condition, particularly when many adenomas develop, when they occur at a young age, or when they appear alongside many other thyroid nodules. Examples include PTEN hamartoma tumor syndrome (Cowden syndrome), DICER1 syndrome, and Carney complex. If an inherited syndrome is suspected, your doctor may refer you for genetic counseling and testing.
How is the diagnosis of follicular adenoma made?
The diagnosis usually begins when a thyroid nodule is found during a physical exam or on imaging. A thyroid ultrasound typically shows a single, well-defined nodule, often with a thin dark rim around it that represents the tumor capsule. Imaging alone cannot reliably distinguish a follicular adenoma from a follicular thyroid carcinoma, as both can look very similar. A fine needle aspiration (FNA) biopsy is often performed next, in which a thin needle is used to remove a small sample of cells from the nodule for examination under the microscope.
An FNA can show that the nodule is made up of follicular cells, but it cannot confirm a diagnosis of follicular adenoma on its own. This is because follicular adenoma and follicular thyroid carcinoma are composed of cells that look almost identical; the difference lies in whether the tumor cells invade the capsule or enter blood vessels, and this can only be assessed when the entire tumor is removed and examined under the microscope. For this reason, FNA results in this setting are usually reported as “follicular neoplasm” or “suspicious for follicular neoplasm,” and surgery is needed to reach a final diagnosis. After surgery, the pathologist examines the whole tumor and its capsule in detail. Because invasion can be very focal, the capsule is often examined extensively, sometimes with additional tissue sections, to confirm that no invasion is present.
Immunohistochemistry is a laboratory test that uses antibodies to detect specific proteins; in follicular adenoma, the tumor cells typically stain for thyroglobulin, TTF-1, and PAX8, confirming their thyroid origin, and the Ki-67 proliferation index (a marker of how quickly cells divide) is low. There are no stains that reliably distinguish a follicular adenoma from a follicular thyroid carcinoma; the diagnosis still depends on whether invasion is present or absent.
What does a follicular adenoma look like under the microscope?
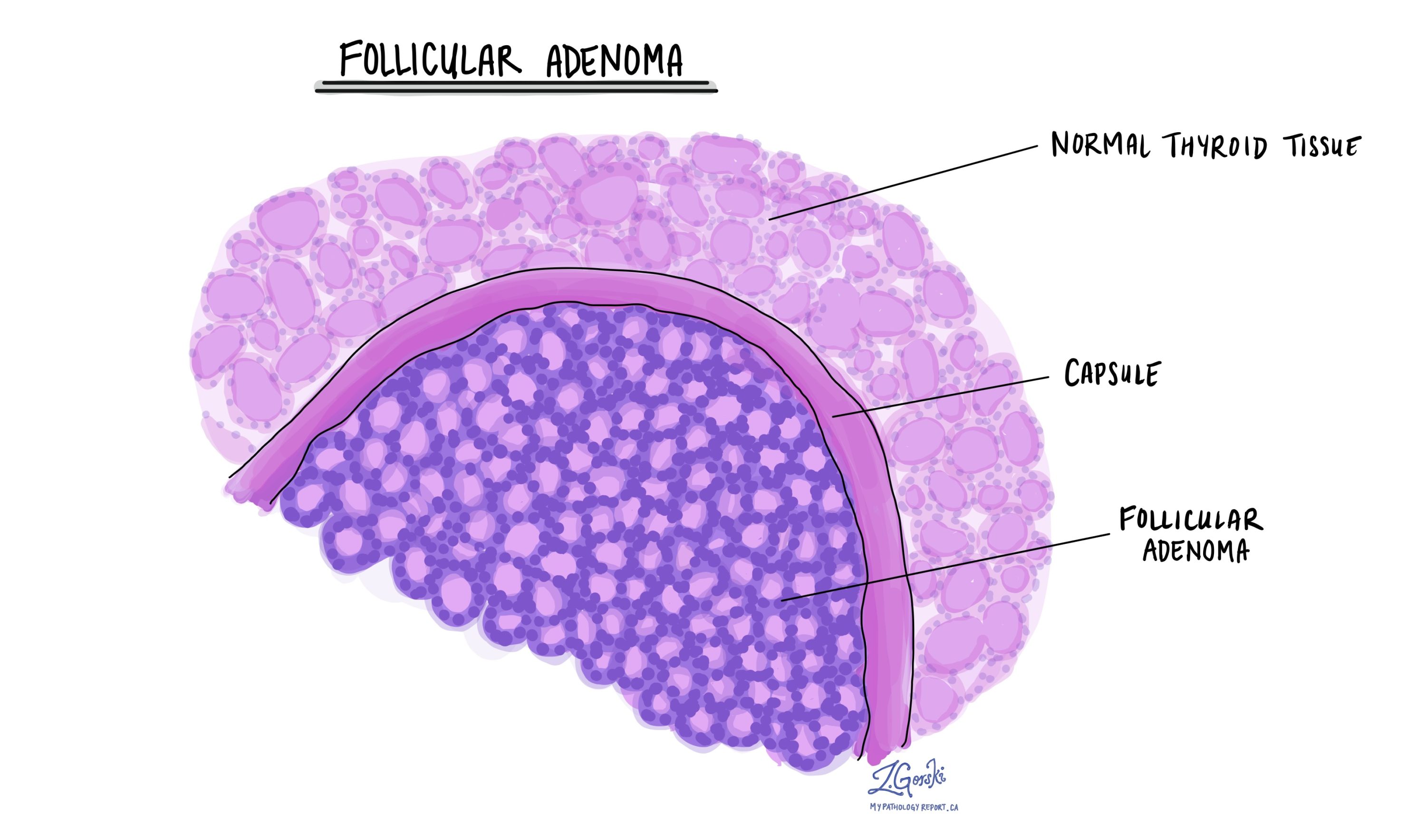
Under the microscope, a follicular adenoma has several characteristic features:
- A complete capsule. A thin, fibrous layer surrounds the entire tumor and clearly separates it from the rest of the thyroid.
- Follicle-forming cells. The tumor is composed of follicular cells arranged in follicles (small, round structures) that may be small, medium, or large. The growth pattern can vary, and sometimes the cells form solid sheets or long cords.
- Bland cell features. The cells resemble normal thyroid follicular cells. Their nuclei are round, have smooth outlines, and lack the changes seen in papillary thyroid carcinoma.
- No invasion. The cells do not invade the capsule or the surrounding thyroid, and no tumor cells are found within blood vessels.
- No aggressive features. There are no areas of tumor cell death (necrosis) and no unusually rapid cell division.
If even a small area of invasion is identified, the diagnosis is changed to follicular thyroid carcinoma.
Biomarkers in follicular adenoma
Biomarker testing is not required to diagnose follicular adenoma. The diagnosis is based on the microscopic appearance of the tumor and the absence of invasion, and no biomarker can reliably make this distinction.
However, follicular adenomas often carry genetic changes such as RAS mutations or PAX8::PPARG rearrangements. These same changes can also be found in follicular thyroid carcinomas, which is why biomarker results alone cannot tell a benign tumor apart from a cancer. In some situations, biomarker testing on an FNA sample before surgery may provide supportive information, but the final diagnosis still depends on microscopic examination of the whole tumor after it has been removed.
What happens after the diagnosis?
The outlook for follicular adenoma is excellent. When the tumor is completely removed, it does not spread to lymph nodes or other organs and does not recur. No additional cancer treatment is needed.
Treatment is usually surgical removal of part or all of the thyroid gland containing the tumor. After surgery, follow-up is focused on routine thyroid monitoring rather than cancer surveillance:
- Thyroid hormone monitoring. Blood tests are used to check thyroid function. Patients who have had part of the thyroid removed can usually keep their remaining thyroid and may not need thyroid hormone medication. Patients who have had a total thyroidectomy will need thyroid hormone replacement for life.
- Clinical follow-up. Regular check-ups with your endocrinologist or family doctor can help identify any new thyroid nodules, particularly if you have other risk factors.
- Genetic evaluation. If your pathology findings or family history suggest an inherited syndrome, you may be referred to a genetic counselor for further evaluation.
Questions to ask your doctor
- Was the entire tumor and its capsule examined under the microscope?
- Was there any sign of invasion, even focal?
- Could my tumor be part of an inherited syndrome? Should I see a genetic counselor?
- Do I need ongoing thyroid hormone monitoring or medication?
- Will I need follow-up imaging or blood tests?
- Is there anything I should watch for, such as new lumps in the neck?
- If I had only part of my thyroid removed, what is the chance of new nodules developing in the remaining thyroid?
Related articles on MyPathologyReport
We are proud to partner with:
![]()