

by Jason Wasserman MD PhD FRCPC
September 16, 2024
SMARCA4-deficient undifferentiated tumour of the lung is a rare and aggressive type of lung cancer. The term “undifferentiated” means that the cancer cells do not look like normal lung cells. The tumour is called “SMARCA4-deficient” because it lacks a functional SMARCA4 gene, which normally helps regulate how cells grow and develop.
What are the symptoms of SMARCA4-deficient undifferentiated tumour?
Patients with SMARCA4-deficient undifferentiated tumours may experience symptoms such as shortness of breath, persistent cough, chest pain, unexplained weight loss, and fatigue. These symptoms are common in many lung diseases, so further testing is needed to make a diagnosis.
What causes SMARCA4-deficient undifferentiated tumour of the lung?
SMARCA4-deficient undifferentiated tumours are strongly associated with heavy smoking, which is believed to be a major risk factor for the development of this type of cancer. Smoking damages the cells in the lungs, leading to mutations in genes like SMARCA4, which can result in uncontrolled cell growth and cancer. Other environmental factors may play a role, but smoking is the most significant contributor.
What other genetic changes may be found in SMARCA4-deficient undifferentiated tumour of the lung?
In addition to SMARCA4 mutations, other genetic changes can be found in this tumour. Mutations in the KRAS gene are common and may contribute to the tumour’s growth. Alterations in STK11 and KEAP1 are also frequently observed and may affect how the tumour behaves and responds to treatment. These genetic changes provide valuable information for understanding the biology of the tumour and may guide treatment options.
How is this diagnosis made?
The diagnosis is made by examining a lung tissue sample under a microscope. The tissue may be a biopsy sample or the entire tumour. Pathologists look for specific features of the tumour cells and may use additional tests such as immunohistochemistry (IHC) or next-generation sequencing (NGS) to confirm the diagnosis.
What are the microscopic features of this tumour?
SMARCA4-deficient undifferentiated tumours are made up of large, round epithelioid cells that often form disorganized sheets. These cells tend to be discohesive (loosely connected) and have large nuclei with a vesicular (open) chromatin pattern and prominent nucleoli. The cells are typically monotonous (they look similar to each other), although some may show mild to moderate pleomorphism (variation in size and shape). Rhabdoid cells – tumour cells that resemble muscle cells – may be seen but are often only present in small areas. The tumours tend to show numerous mitotic figures (evidence of rapid cell division) and necrosis (dead tissue).
What additional tests may be performed to confirm the diagnosis?
Two main types of tests are often performed to confirm a diagnosis of SMARCA4-deficient undifferentiated tumour: immunohistochemistry (IHC) and next-generation sequencing (NGS).
Immunohistochemistry
Immunohistochemistry (IHC) is a technique used to detect specific proteins in the tumour cells. In SMARCA4-deficient tumours, the SMARCA4 protein is typically absent or significantly reduced. Other markers that may be positive include CD34, SOX2, SALL4, synaptophysin, and cytokeratins. These markers help confirm the diagnosis and provide additional information about the tumour’s characteristics.
Next-generation sequencing
Next-generation sequencing (NGS) is used to identify mutations in the tumour’s DNA, particularly in the SMARCA4 gene. This test can confirm the presence of a mutation in SMARCA4, which explains the loss of this important protein. Sequencing may also detect other mutations, such as those in the KRAS, STK11, and KEAP1 genes, commonly associated with this type of cancer.
Pleural invasion
Pleural invasion refers to the spread of cancer cells into the pleura, the thin layer of tissue surrounding the lungs and lining the inside of the chest cavity. There are two layers of the pleura: the visceral pleura, which sticks to the lungs, and the parietal pleura, which lines the chest wall and diaphragm. Pleural invasion by lung cancer means the tumour has grown beyond the lung tissue and into the surrounding pleural layers.
Pleural invasion is important both for determining the pathologic stage and for prognosis:
- Tumour stage: Pleural invasion is a significant factor in determining the lung cancer stage. Tumours that invade the pleura are considered more advanced than those confined to the lung parenchyma (the functional tissue of the lung). According to the TNM classification system used for staging lung cancer, pleural invasion may increase the T category of the tumour, which signifies tumour size and extent. For example, a tumour that invades the visceral pleura might be classified as T2. In contrast, invasion into the parietal pleura or involvement of pleural effusion (fluid accumulation) could lead to a higher classification.
- Prognosis: Patients with lung cancer that has invaded the pleura generally have a poorer prognosis than those without pleural involvement. This is because pleural invasion reflects a more aggressive tumour that is more likely to spread and cause complications, such as pleural effusion, which can impair lung function and lead to symptoms like chest pain, cough, and shortness of breath.
Lymphovascular invasion
Lymphovascular invasion refers to the spread of cancer cells into a blood vessel or lymphatic channel. Blood vessels are long, thin tubes that carry blood around the body. Lymphatic channels are similar to small blood vessels except that they carry a fluid called lymph instead of blood. The lymphatic channels connect with small immune organs called lymph nodes throughout the body. Lymphovascular invasion is important because once inside a blood vessel or lymphatic space, cancer cells can spread to lymph nodes or other body parts, such as the liver or bones.

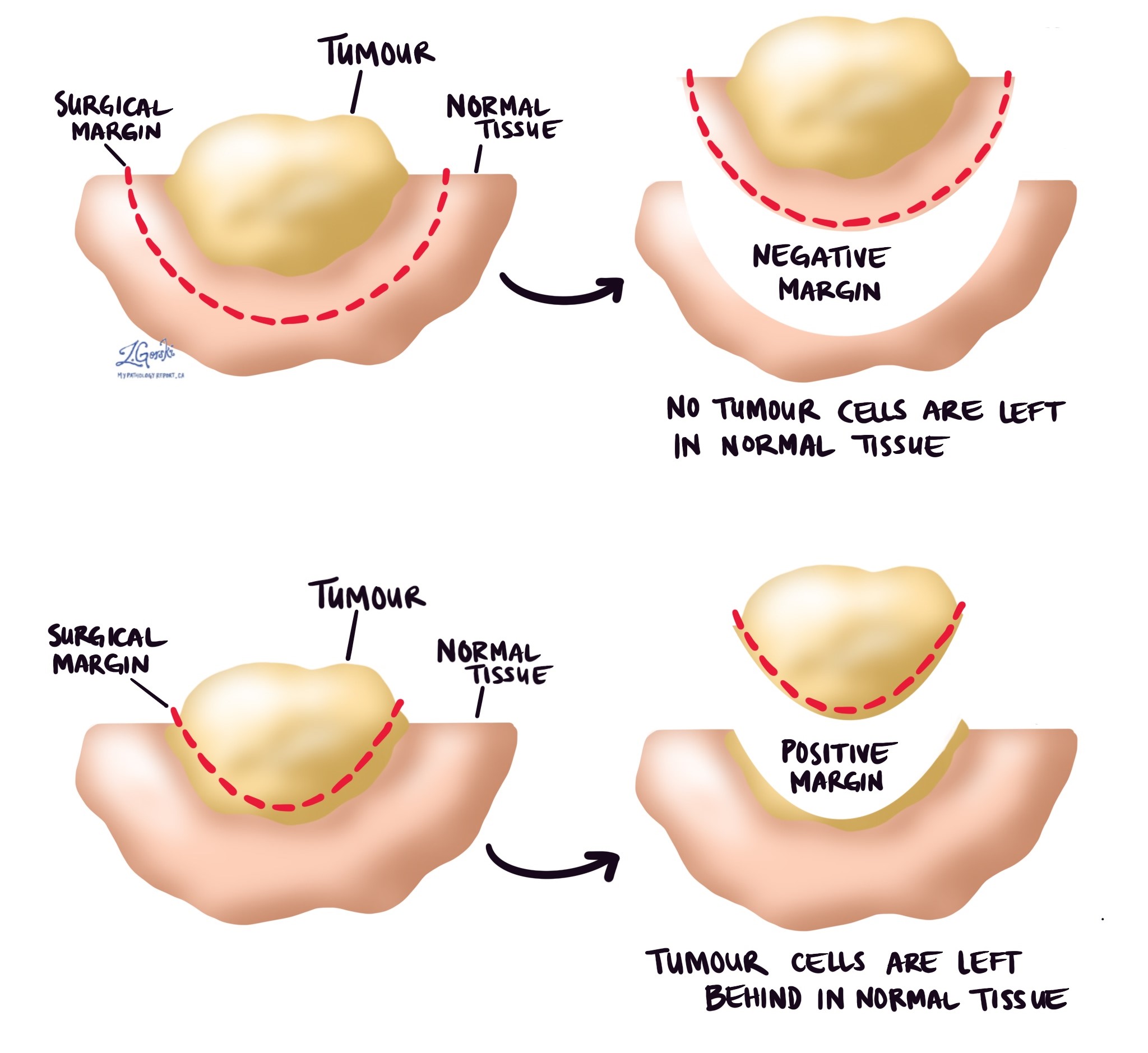
Margins
In pathology, a margin is the edge of a tissue cut when removing a tumour from the body. The margins described in a pathology report are very important because they tell you if the entire tumour was removed or if some of the tumour was left behind. The margin status will determine what (if any) additional treatment you may require.
Pathologists carefully examine the margins to look for tumour cells at the cut edge of the tissue. If tumour cells are seen at the cut edge of the tissue, the margin will be described as positive. If no tumour cells are seen at the cut edge of the tissue, a margin will be described as negative. Even if all of the margins are negative, some pathology reports will also measure the closest tumour cells to the cut edge of the tissue.
A positive (or very close) margin is important because it means that tumour cells may have been left behind in your body when the tumour was surgically removed. For this reason, patients with a positive margin may be offered another surgery to remove the rest of the tumour or radiation therapy to the area of the body with the positive margin.
Lymph nodes
Lymph nodes are small immune organs found throughout the body. Cancer cells can spread through small lymphatic vessels from tumours to lymph nodes. For this reason, lymph nodes are commonly removed and examined under a microscope to look for cancer cells. The movement of cancer cells from the tumour to another part of the body, such as a lymph node, is called metastasis.
Lymph nodes from the neck, chest, and lungs may be removed at the same time as the tumour. These lymph nodes are divided into areas called stations. There are 14 different stations in the neck, chest, and lungs (see picture below).
If any lymph nodes were removed from your body, they will be examined under the microscope by a pathologist, and the results of this examination will be described in your report. Most reports will include the total number of lymph nodes examined, where the lymph nodes were found in the body, and the number (if any) that contain cancer cells. If cancer cells were seen in a lymph node, the size of the largest group of cancer cells (often described as “focus” or “deposit”) will also be included.
The examination of lymph nodes is important for two reasons. First, this information determines the pathologic nodal stage (pN). Second, finding cancer cells in a lymph node increases the risk that cancer cells will be found in other parts of the body in the future. As a result, your doctor will use this information when deciding if additional treatment, such as chemotherapy, radiation therapy, or immunotherapy, is required.

Pathologic stage (pTNM)
The pathologic stage for SMARCA4-deficient undifferentiated tumour of the lung is based on the TNM staging system, an internationally recognized system created by the American Joint Committee on Cancer. This system uses information about the primary tumour (T), lymph nodes (N), and distant metastatic disease (M) to determine the complete pathologic stage (pTNM). Your pathologist will examine the tissue submitted and give each part a number. In general, a higher number means a more advanced disease and a worse prognosis.
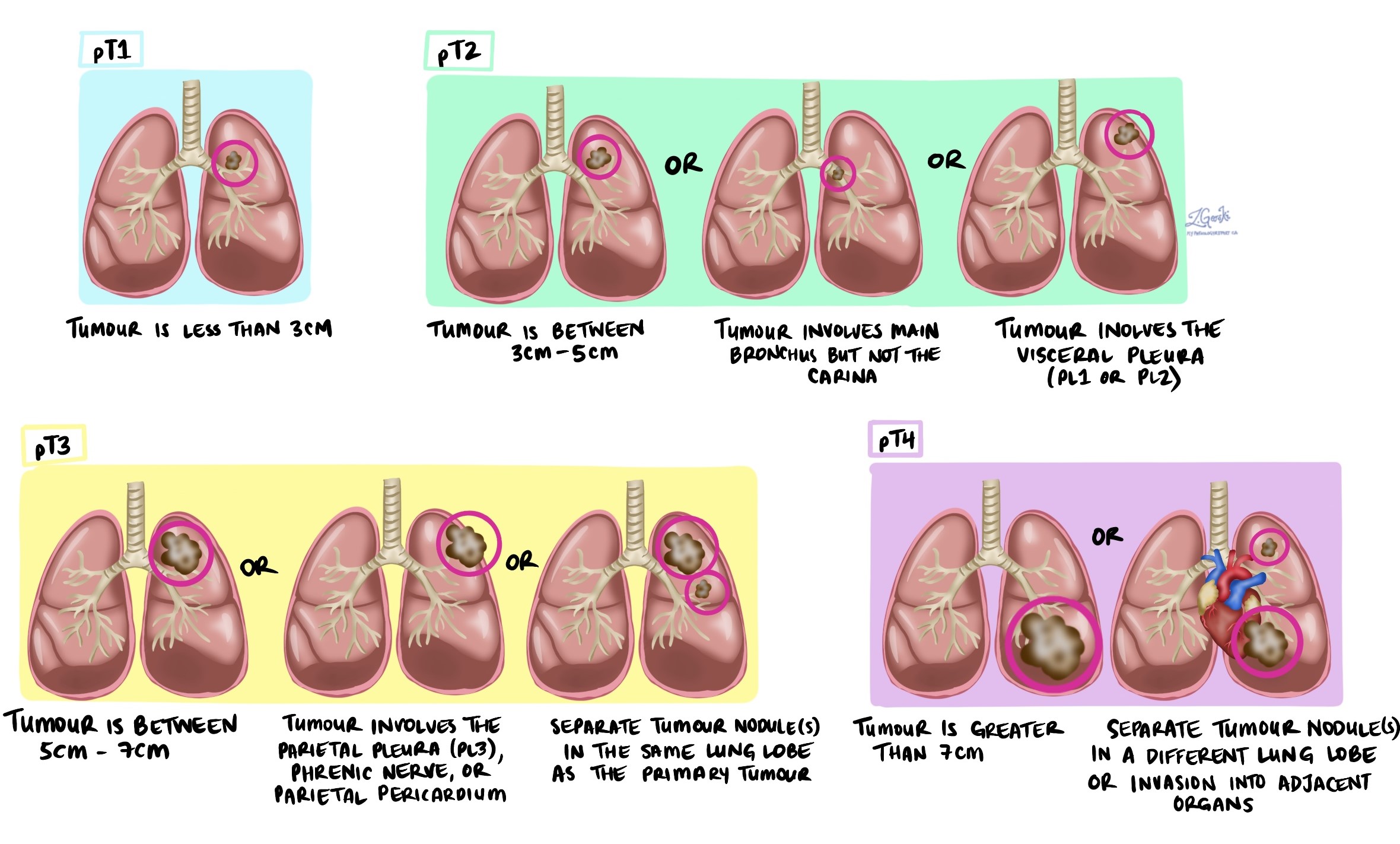
Tumour stage (pT)
SMARCA4-deficient undifferentiated tumour of the lung is given a tumour stage between 1 and 4 based on the size of the tumour, the number of tumours found in the tissue examined, and whether the tumour has broken through the pleural or has spread to organs around the lungs.
Nodal stage (pN)
SMARCA4-deficient undifferentiated tumour of the lung is given a nodal stage between 0 and 3 based on the presence or absence of cancer cells in a lymph node and the location of the lymph nodes that contain cancer cells.
- NX – No lymph nodes were sent for pathologic examination.
- N0 – No cancer cells were found in any lymph nodes examined.
- N1 – Cancer cells were found in at least one lymph node inside or around the large airways leading into the lung. This stage includes stations 10 through 14.
- N2 -Cancer cells were found in at least one lymph node from the tissue in the middle of the chest and around the large airways. This stage includes stations 7 through 9.
- N3 – Cancer cells were found in the neck or lymph nodes on the side of the body opposite (contralateral) to the tumour. This stage includes stations 1 through 6.
Treatment effect
Treatment effect is described in your report only if you received either chemotherapy or radiation therapy before surgery to remove the tumour. To determine the treatment effect, your pathologist will measure the amount of living (viable) tumour and express that number as a percentage of the original tumour. For example, if your pathologist finds 1 cm of viable tumour and the original tumour was 10 cm, the percentage of viable tumour is 10%.
What is the prognosis for SMARCA4-deficient undifferentiated tumour?
SMARCA4-deficient undifferentiated tumours are aggressive, meaning they grow and spread quickly. Because of this, the prognosis can be challenging, with limited treatment options available. The stage of the tumour at diagnosis, along with other factors such as the presence of genetic mutations, plays a role in determining the patient’s outlook. Research into targeted therapies and immunotherapies offers hope for improving outcomes in the future.
Learn more pathology
Atlas of pathology
We are proud to partner with:
![]()