

by Jason Wasserman MD PhD FRCPC and Zuzanna Gorski MD FRCPC
May 14, 2026
High grade squamous intraepithelial lesion (HSIL) is a precancerous condition of the cervix caused by infection with human papillomavirus (HPV). It is composed of squamous cells infected and altered by the virus. These abnormal cells are found in the transformation zone, the part of the cervix where glandular cells are gradually replaced by squamous cells. HSIL is not cancer, but it is considered a serious precancerous change because it can progress over time to a type of cervical cancer called HPV-associated squamous cell carcinoma if it is not treated.
Another name for HSIL is cervical intraepithelial neoplasia (CIN). CIN is divided into three levels based on severity: CIN1, CIN2, and CIN3. HSIL corresponds to CIN2 and CIN3, which are considered the high-grade changes. The lower-grade form, CIN1, is called low grade squamous intraepithelial lesion (LSIL) and behaves quite differently. This article will help you understand the findings in your pathology report — what each term means and why it matters for your care.
What causes HSIL?
HSIL is caused by persistent infection with high-risk types of HPV. HPV is a very common virus that spreads through skin-to-skin contact, including sexual contact. The high-risk types most often linked to HSIL and cervical cancer include HPV16 and HPV18, along with HPV31, 33, 45, 52, and 58. These viruses produce proteins that interfere with the systems controlling normal cell growth, and over time, they can cause squamous cells to grow abnormally.
Most HPV infections do not lead to HSIL. In the majority of people, the immune system clears the virus within one to two years, and the cellular changes resolve along with it. Only a small percentage of infections persist in the cervix long enough to cause precancerous changes. Several factors make persistent infection and progression to HSIL more likely:
- Persistent infection with high-risk HPV — Infections that last two years or longer are the most important risk factor for HSIL.
- A weakened immune system — Conditions such as HIV infection, organ transplantation, or long-term immunosuppressive therapy make it harder for the body to clear the virus.
- Cigarette smoking — Smoking damages cervical cells and makes them more vulnerable to HPV-related changes.
- Long-term use of oral contraceptives — Has been associated with a modestly increased risk in some studies.
- Lack of regular cervical cancer screening — Without screening, precancerous changes can go undetected for many years.
What are the symptoms?
Most people with HSIL have no symptoms. The abnormal cells in HSIL are confined to the surface lining of the cervix and do not invade deeper tissue, so they typically do not cause bleeding, pain, or discharge. For this reason, HSIL is almost always discovered through routine cervical cancer screening rather than because of symptoms.
When symptoms do occur, they may include abnormal vaginal bleeding (such as bleeding after intercourse or between periods), unusual vaginal discharge that may be watery or blood-tinged, or pelvic discomfort, though pelvic pain is uncommon. These symptoms are not specific to HSIL and can result from many other less serious conditions. Because HSIL itself rarely causes noticeable symptoms, regular Pap testing and HPV testing remain the most reliable way to find it before it has the chance to progress.
How is the diagnosis made?
HSIL is most often first suspected when a Pap test shows abnormal squamous cells, or when an HPV test is positive for high-risk types. When either result is found, the next step is typically a colposcopy: an examination of the cervix using a colposcope, a magnifying instrument that allows the doctor to look closely at its surface. During colposcopy, a small tissue sample called a biopsy is taken from any area that looks abnormal and sent to the laboratory for examination. A second sample, called an endocervical curettage, may also be collected from inside the cervical canal to look for changes that cannot be fully seen with the colposcope.
Under the microscope, the pathologist identifies HSIL by examining how much of the surface lining of the cervix (the epithelium) has been replaced by abnormal squamous cells. In HSIL, the abnormal cells extend through at least two-thirds of the thickness of the epithelium and lack the normal maturation seen in healthy squamous cells.
To support the diagnosis, additional tests are often performed. A protein stain called p16, performed by immunohistochemistry, almost always shows strong, continuous “block-type” staining in HSIL because cells infected with high-risk HPV produce large amounts of this protein. This staining pattern supports the diagnosis of HSIL and helps distinguish it from LSIL and other conditions that can look similar under the microscope. When the diagnosis is uncertain, a test called in situ hybridization (ISH) can also be used to detect HPV genetic material directly inside the cells, confirming whether the abnormal cells are HPV-driven and sometimes identifying the specific HPV type.
What does HSIL look like under the microscope?
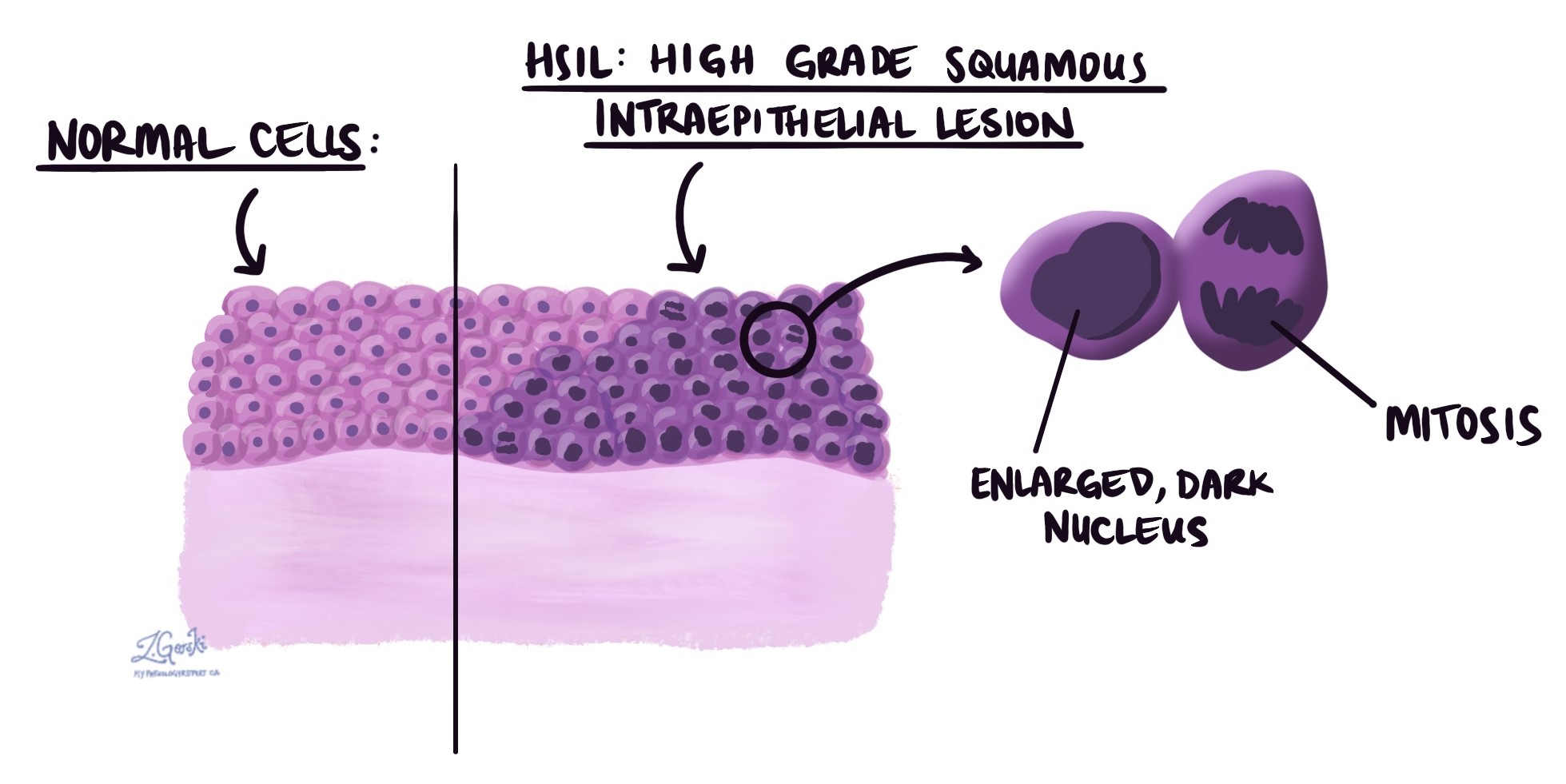
Under the microscope, HSIL is made up of abnormal squamous cells that are darker and larger than normal and that fill the upper two-thirds or full thickness of the cervical surface lining. The cells remain confined to the epithelium and have not invaded deeper tissue, which is what makes HSIL precancerous rather than cancer. Several features help the pathologist recognize HSIL:
- Dark, enlarged nuclei — The nuclei (the parts of the cells that contain genetic material) appear darker than normal, a feature called hyperchromasia.
- Loss of normal maturation — Healthy squamous cells become progressively flatter and more mature as they move toward the surface. In HSIL, this orderly maturation is lost, and immature-looking cells extend high into the epithelium.
- High nuclear-to-cytoplasmic ratio — The cells have less cytoplasm (the body of the cell) relative to the size of the nucleus, making the overall appearance dark and crowded.
- Many mitotic figures — Mitotic figures (dividing cells) are numerous, often including abnormal forms called atypical mitotic figures. Many of these dividing cells are seen above the lower one-third of the epithelium, which is where dividing cells should normally be confined.
- Occasional koilocytes — Koilocytes are cells with irregular nuclei and a clear space (or “halo”) around the nucleus, caused by HPV infection. They are more typical of LSIL but may also be present in HSIL.
How is HSIL different from LSIL?
Both HSIL and LSIL are caused by HPV infection of the cervix, but they differ in how the cells look under the microscope, how likely they are to resolve on their own, and how they are managed.
LSIL (which corresponds to CIN1) is a low-grade change in which the abnormal squamous cells are confined to the lower one-third of the epithelium. The risk of LSIL progressing to cancer is low, and most cases resolve on their own as the immune system clears the underlying HPV infection. For this reason, LSIL is usually managed with close monitoring rather than immediate treatment.
HSIL (which corresponds to CIN2 and CIN3) is a high-grade change in which the abnormal cells extend through at least two-thirds of the epithelium. HSIL is much less likely to resolve on its own and carries a meaningful risk of progressing to cervical cancer over time if left untreated. Because of this risk, the standard approach when HSIL is confirmed on biopsy is to remove the abnormal area.
Surgical margins
A margin is the cut edge of tissue that was removed during an excision procedure. After surgery, the pathologist examines the margins under the microscope to determine whether any HSIL cells are present at the cut edge. Margins are reported only in excision specimens, such as a loop electrosurgical excision procedure (LEEP) or cone biopsy. They are not reported on Pap tests or small biopsies, which are not intended to remove the entire lesion.
- Negative margin — No HSIL cells are present at the cut edge of the tissue. This result suggests that the abnormal area was completely removed, and it is the most reassuring outcome.
- Positive margin — HSIL cells are present at the cut edge. This means some abnormal cells may still remain in the cervix, increasing the risk that HSIL could recur and prompting the gynecologic team to discuss either repeat excision or closer follow-up.
Three margin locations are assessed in cervical excision specimens:
- Endocervical margin — The inner edge of the specimen, closest to the uterus. Involvement of this margin is particularly significant because abnormal cells may remain high in the endocervical canal, where they are difficult to detect on follow-up screening.
- Ectocervical margin — The outer edge of the specimen, closest to the vagina.
- Stromal margin — The deep edge, corresponding to the wall of the cervix beneath the removed tissue.
What is the prognosis?
With treatment, the outlook for HSIL is excellent in most cases. The majority of patients are cured after a single excision procedure, and the risk of progressing to cervical cancer drops substantially once the abnormal tissue has been removed. Several features in the pathology report influence the chance of recurrence or progression:
- Margin status after excision — Negative margins are associated with a low recurrence rate, generally in the range of 5 to 10% over the years following treatment. Positive margins, especially at the endocervical edge, are associated with a substantially higher risk of residual or recurrent disease.
- Clearance of HPV after treatment — A negative HPV test six to twelve months after treatment is one of the strongest indicators that the underlying infection has been cleared and the risk of recurrence is low. Persistent HPV infection after treatment is the most important predictor of recurrence.
- Grade of the lesion — The risk of progression to cancer without treatment is meaningfully higher for CIN3 than for CIN2. With treatment, however, both are managed similarly and the outlook is similar.
- Immune status — People with weakened immune systems (HIV infection, organ transplant, long-term immunosuppression) are at higher risk of recurrence and may require closer surveillance.
- Risk of progression without treatment — When HSIL is not treated, studies indicate that a meaningful proportion of CIN3 lesions progress to invasive cervical cancer over a period of years to decades. CIN2 has a lower but still meaningful rate of progression, and a notable percentage of CIN2 lesions also resolve spontaneously, particularly in younger patients.
What happens after this diagnosis?
Once HSIL is confirmed on biopsy, the gynecologic team will discuss the options for managing the abnormal area. Because HSIL carries a meaningful risk of progressing to cervical cancer over time, the standard approach is to remove the abnormal tissue. The choice of procedure depends on the size and location of the lesion, your age, your wish to preserve fertility, and your overall medical history.
Options the team may consider include:
- Loop electrosurgical excision procedure (LEEP) — A thin wire loop heated by an electrical current removes a layer of cervical tissue, including the transformation zone. LEEP is the most common procedure for HSIL because it removes the abnormal area while also providing tissue that the pathologist can fully examine for margin status and any unexpected findings.
- Cold knife cone biopsy (conization) — A cone-shaped portion of the cervix is surgically removed in the operating room. This option is often considered when a larger or deeper specimen is needed, when the abnormal area extends high into the endocervical canal, or when there is concern that an early cancer may also be present.
- Ablative procedures (cryotherapy, laser ablation) — These destroy the abnormal tissue rather than removing it. They are used less commonly for HSIL because they do not provide tissue for pathology examination, which means margin status cannot be assessed and a small underlying cancer could potentially be missed.
- Close monitoring without immediate treatment — In selected cases, particularly in younger patients with CIN2 who wish to preserve fertility, surveillance with repeat Pap and HPV testing rather than immediate excision may be discussed. The reason this option is sometimes considered is that a meaningful proportion of CIN2 lesions resolve spontaneously, especially in people under age 25.
After treatment, ongoing surveillance is essential to detect any recurrence early. The standard follow-up schedule includes Pap testing and HPV testing six months after treatment, with additional testing at 12 and 24 months. After two consecutive negative results, most patients can return to routine screening intervals. Your doctor or gynecologic specialist will tailor this schedule based on your specific pathology results, margin status, HPV test results, and overall medical history.
Questions to ask your doctor
- Did my biopsy confirm HSIL, and was it described as CIN2 or CIN3?
- Was my sample tested for p16, and what did the result show?
- Did my sample test positive for high-risk HPV, and if so, which type?
- What treatment options would you discuss with me, and what are the benefits and drawbacks of each?
- I want to preserve my fertility — how does that affect the choice of procedure?
- If close monitoring is an option for me, what would the surveillance schedule look like?
- If I have a procedure, were the surgical margins clear, and what do my margin results mean for next steps?
- What is my chance of HSIL coming back after treatment?
- How often will I need follow-up Pap tests and HPV testing, and for how long?
- When can I return to routine cervical cancer screening?
- Should I consider HPV vaccination if I have not already been vaccinated?
- What symptoms should prompt me to contact you between appointments?
Related articles on MyPathologyReport.com
- Cervical intraepithelial neoplasia (CIN)
- Low grade squamous intraepithelial lesion (LSIL) of the cervix
- Adenocarcinoma in situ (AIS) of the cervix
- HPV-associated squamous cell carcinoma of the cervix
- HPV-independent squamous cell carcinoma of the cervix
- ASC-H of the cervix
- ASC-US of the cervix
- Negative for intraepithelial lesion or malignancy (NILM)
- Pap test
- Human papillomavirus (HPV)
- High-risk HPV
- p16
We are proud to partner with:
![]()