

By Jason Wasserman MD PhD FRCPC
December 12, 2024
This article is designed to help you understand your pathology report for well differentiated neuroendocrine tumour of the small intestine. Each section explains an important aspect of the diagnosis and what it means for you.
What is a well differentiated neuroendocrine tumour?
A well differentiated neuroendocrine tumour (NET) is a type of small intestinal cancer that starts in neuroendocrine cells. These cells are found throughout the body, including the small intestine, and help regulate various functions by producing hormones. Unlike poorly differentiated neuroendocrine carcinomas, well differentiated neuroendocrine tumours grow more slowly and are less aggressive.
The small intestine, where these tumours are found, is part of the digestive system between the stomach and the large intestine. It is divided into three sections:
- Duodenum – This is the first part of the small intestine, which receives partially digested food from the stomach. It also includes the ampulla of Vater, a small opening where bile and pancreatic fluids enter the intestine to help digest food. The ampulla is a common location for these neuroendocrine tumours.
- Jejunum – This is the middle section of the small intestine where most nutrient absorption occurs.
- Ileum – This is the final section of the small intestine, which absorbs vitamin B12 and bile acids.
Well differentiated neuroendocrine tumours can occur in any part of the small intestine. More than 95% of duodenal tumours are found in the first or second part of the duodenum, with most in the ampullary region. Tumours that produce a hormone called somatostatin occur almost exclusively in the ampullary area. Tumours outside the duodenum are predominantly located in the distal ileum, with only 11% originating in the jejunum. Rarely enterochromaffin-cell (ECL) tumours can arise in Meckel diverticula.
What are the symptoms of a well differentiated neuroendocrine tumour in the small intestine?
Symptoms of well differentiated neuroendocrine tumours depend on the tumour’s location and whether it produces hormones. Many small intestinal neuroendocrine tumours do not produce symptoms and are found incidentally during medical exams or procedures.
- Non-functioning tumours (those that do not produce hormones): Symptoms occur due to the tumour’s size or location and include intestinal obstruction, jaundice, or abdominal pain.
- Functioning tumours (those that produce hormones): Symptoms depend on the type of hormone secreted.
- Carcinoid syndrome: Diarrhoea, flushing, bronchospasms, and heart valve disease (occurs only if the tumour has spread to the liver).
- Zollinger–Ellison syndrome: Excessive stomach acid production leading to peptic ulcers and diarrhoea.
- Somatostatinoma syndrome (rare): Diabetes, diarrhoea, gallstones, and anaemia.
What causes a well differentiated neuroendocrine tumour in the small intestine?
Most well differentiated neuroendocrine tumours are sporadic and occur without a known inherited cause. However, some are linked to genetic conditions:
- Hereditary syndromes: Some tumours arise in patients with multiple endocrine neoplasia type 1 (MEN1) or neurofibromatosis type 1 (NF1).
- Rare genetic mutations: Mutations in genes like EPAS1 have been linked to specific neuroendocrine tumours.
- Family history: About 5% of patients with jejunal or ileal neuroendocrine tumours have a close relative with a similar tumour, although the genetic cause is usually unknown.
How is this diagnosis made?
The diagnosis of a well differentiated neuroendocrine tumour is typically made after a biopsy or surgical removal of the tumour. A pathologist examines the tissue under a microscope and may use additional tests, such as immunohistochemistry, to confirm the diagnosis and determine the grade.
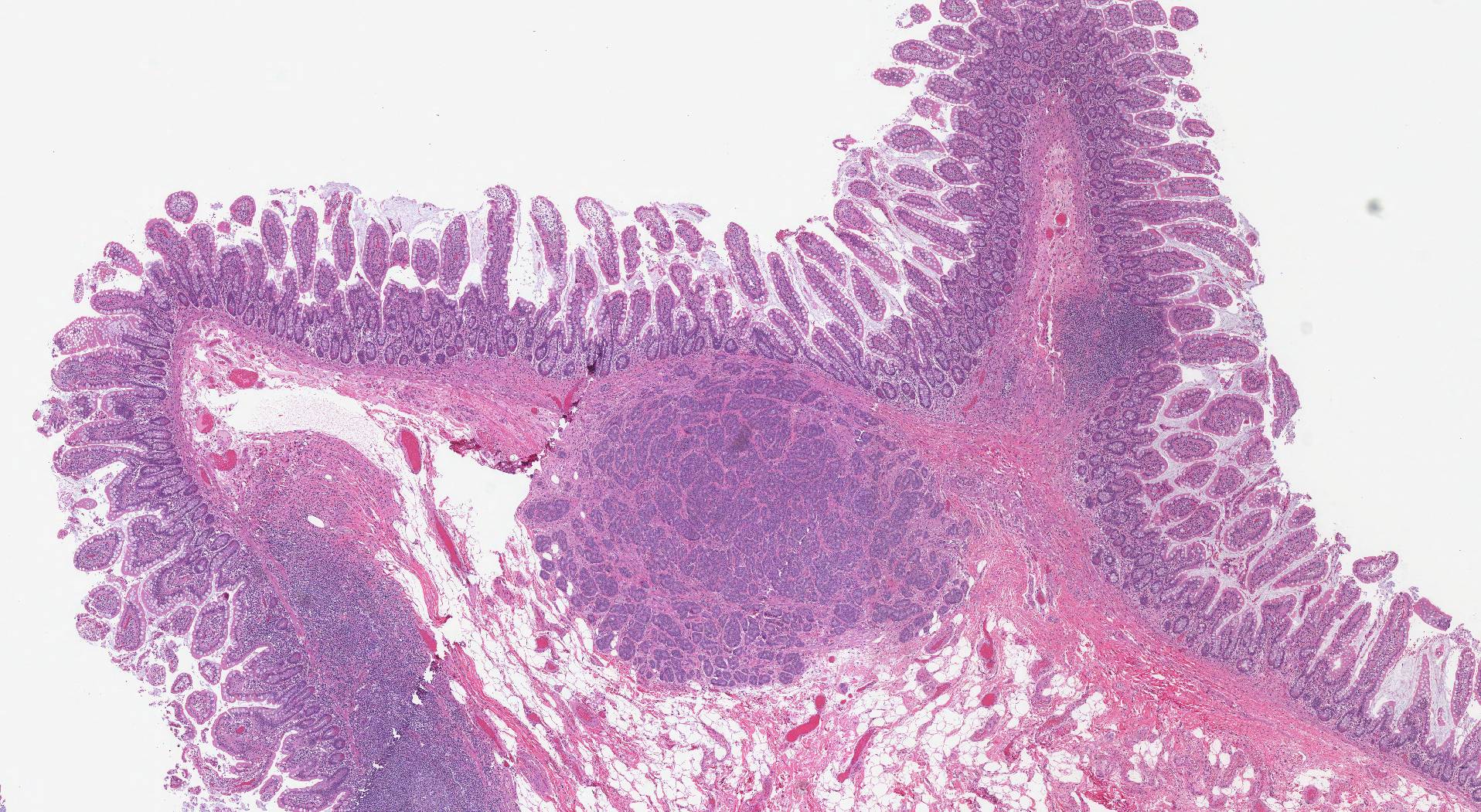
Microscopic features of this tumour
Well differentiated neuroendocrine tumours of the small intestine are composed of uniform neuroendocrine cells with round to oval nuclei. These nuclei have finely granular chromatin, a feature typical of neuroendocrine tumours found in other parts of the body. The cells show little variation in size and shape.
Tumours producing gastrin (G-cell tumours) in the duodenum often display a trabecular growth pattern. In contrast, somatostatin-producing tumours (D-cell tumours) found in the ampullary region tend to grow in tubuloglandular structures and may include psammoma bodies, which are small, round collections of calcium. Tumours that produce serotonin (EC-cell tumours) in the jejunum or ileum are typically organized into nests of tumour cells surrounded by a layer of palisaded cells, and these nests may occasionally form small gland-like structures called pseudoglands. In areas of tissue scarring or sclerosis, the growth pattern of the tumour can change, with tumour cells forming single-file arrangements or small nests.
Immunohistochemistry
Immunohistochemistry is a special test that pathologists use to identify specific proteins in tumour cells. This test helps confirm the diagnosis of a well differentiated neuroendocrine tumour and provides information about the tumour’s behaviour.
Most neuroendocrine tumours in the small intestine produce general neuroendocrine markers, such as chromogranin A and synaptophysin, which help pathologists identify these tumours. However, somatostatin-producing tumours are less likely to express chromogranin A. Tumours in the ileum that produce serotonin often test positive for CDX2 and SSTR2A. Keratin staining, including CK8/18, distinguishes neuroendocrine tumours from other tumour types, such as paragangliomas.
WHO grade
Well differentiated neuroendocrine tumours in the small intestine are divided into three grades based on how quickly the tumour cells divide. This information is important because higher-grade tumours (grades 2 and 3) are more likely to spread to other body parts. The grade can only be determined after examining the tumour under a microscope.
Pathologists measure the number of dividing tumour cells, called mitotic figures, to determine the grade. The number of mitotic figures is typically counted in an area measuring 2 mm2. To highlight cells capable of dividing, a special test called immunohistochemistry for Ki-67 may also be performed. The results are used to calculate the proliferative index (the percentage of tumour cells producing Ki-67).
- Grade 1 (G1): Mitotic rate of less than 2 per 2 mm2 or Ki-67 index of less than 3%.
- Grade 2 (G2): Mitotic rate between 2 and 20 per 2 mm2 or Ki-67 index between 3% and 20%.
- Grade 3 (G3): Mitotic rate greater than 20 per 2 mm2 or Ki-67 index greater than 20%.
Tumour extension
Well differentiated neuroendocrine tumours begin in the mucosa on the inside surface of the small intestine. As the tumour grows, it can invade deeper into the wall of the organ.
The small intestine has several layers:
- Mucosa: The innermost layer where most tumours begin. The mucosa includes the epithelium, lamina propria, and muscularis mucosae.
- Submucosa: A supportive layer beneath the mucosa.
- Muscularis propria: A thick muscle layer that helps the small intestine contract.
- Subserosa and serosa: Outer layers that protect the small intestine and separate it from nearby organs.
The depth of invasion is important because tumours that extend deeper into the small intestinal wall are more likely to spread to other organs such as the pancreas, stomach, and lymph nodes. Tumour extension is also used to determine the pathologic tumour stage (pT).
Margins
In pathology, a margin is the edge of tissue removed during tumour surgery. The margin status in a pathology report is important as it indicates whether the entire tumour was removed or if some was left behind. This information helps determine the need for further treatment.
Pathologists typically assess margins following a surgical procedure, such as an excision or resection, that removes the entire tumour. They aren’t usually evaluated after a biopsy, which removes only part of the tumour. The number of margins reported and their size—how much normal tissue is between the tumour and the cut edge—vary based on the tissue type and tumour location.
Pathologists examine margins to check if tumour cells are at the tissue’s cut edge. A positive margin, where tumour cells are found, suggests that some cancer may remain in the body. In contrast, a negative margin, with no tumour cells at the edge, suggests the tumour was entirely removed. Some reports also measure the distance between the nearest tumour cells and the margin, even if all margins are negative.

Pathologic stage
The TNM staging system is used to describe the size and extent of the tumour (T), the involvement of lymph nodes (N), and the presence of metastasis (M). Staging helps doctors understand how advanced the tumour is, guide treatment decisions, and predict outcomes.
Duodenal tumours
- Tumour stage (T):
- T1: Tumour invades mucosa or submucosa and is ≤ 1 cm in size.
- T2: Tumour invades the muscularis propria or is > 1 cm in size.
- T3: Tumour invades the pancreas or peripancreatic tissue.
- T4: Tumour invades the peritoneum or nearby organs.
- Nodal stage (N):
- N0: No tumour involvement of regional lymph nodes.
- N1: Tumour involvement of regional lymph nodes.
Jejunal and ileal tumours
- Tumour stage (T):
- T1: Tumour invades mucosa or submucosa and is ≤ 1 cm in size.
- T2: Tumour invades the muscularis propria or is > 1 cm in size.
- T3: Tumour invades through the muscularis propria into the subserosa.
- T4: Tumour invades the peritoneum or nearby organs.
- Nodal stage (N):
- N0: No tumour involvement of regional lymph nodes.
- N1: Tumour involvement of fewer than 12 regional lymph nodes.
- N2: Tumour involvement of large mesenteric masses (> 2 cm) and/or extensive nodal deposits (≥ 12 nodes), especially those encasing the superior mesenteric vessels.
What is the prognosis for a person diagnosed with a well differentiated neuroendocrine tumour of the small intestine?
The prognosis for a patient diagnosed with a well differentiated neuroendocrine tumour of the small intestine depends on the tumour’s grade and stage:
- Localized tumours: Patients with tumours confined to the small intestine often have a 5-year survival rate of 70–100%.
- Advanced tumours: Patients with distant metastases (e.g., liver involvement) have a 5-year survival rate of 35–60%.
Factors like lymphovascular invasion (spread of tumour cells into blood or lymph vessels) or perineural invasion (spread into nerves) can increase the risk of recurrence. Despite this, many patients with advanced disease live for years due to the slow growth of these tumours.
We are proud to partner with:
![]()